Top
INDEX
Incidents
- About: Dr. Stan Houston, Univ of Alberta, Faculty of Medicine.
MEDIA
- Quotes: CBC News --- Posted: Jul 19, 2017
- Quotes: CBC Radio -- Posted: Jun 07, 2019
- Quotes: CBC News --- Posted: Jul 25, 2019
- Quotes: Star Calgary - Thur., July 25, 2019
- Quotes: CBC News --- Posted: Jan 23, 2020
- -About: Echinococcus multilocularis.
- Article: Echinococcus multilocularis Infection, Southern Ontario, Canada.
- Article: Cutaneous Disease as the First Manifestation of Cystic Echinococcosis.
- Article: Superinfection of a Dead Hepatic Echinococcal Cyst w/ a Cutaneous Fistulization.
- Article: Echinococcus multilocularis: An Emerging Pathogen in ...
- Article: Alveolar echinococcosis (AE), USA CDC.
- Article: Echinococcus, Healthline.
- Article: Parasites of the Liver � epidemiology, diagnosis .. **
- Article: Echinococcosis, WHO World Health Organization.
- Article: A multiplex PCR for .. detection of .. Echinococcus multilocularis ..
- Article: IDEXX introduces .. new Echinococcus RealPCR Panel (2019).
- Article: Toxocariasis, Hydatid Disease of the Lung, .. and Pulmonary .. (2012)
- Article: Parasites in Food: Occurrence and Detection. (2016)
- Article: Solitary Lucent Defect, Parasitic Cysts. (2019)
- Article: Echinococcus multilocularis Revisited. (2001)
- Article:
- - Research: HPA (hypothalamic-pituitary-adrenal) axis.
- Symptoms: Possible indicators of infestation.
- .
- .
- .
- Testing: Serologic tests.
- Testing: Serological and imaging tests.
- Testing: blood tested for the presence of antibodies.
- Testing: Laboratory tests ... ultrasound ....
- Testing: Radiography of lungs & other organs ...
- Testing: Medical tests to diagnose your infection.
- Testing: the immunochromatographic VIRapid� HYDATIDOSIS test (2015)
- Testing: Diagnostics ... serology versus ultrasonography (2014)
- Testing: ECHNO, Echinococcus Antibody, IgG, Serum Test. (2016)
- Testing: LabCorp Burlington, NC, Echinococcus Antibody. (2021)
- Testing:
- Testing:
Why Echinococcus multilocularis is usually NOT found.
- -- Article: Lichens and People ....
- Treatment for Skin Lichenization.
- - Product: Creme Complete, Perrin Naturals.
- - Product: Taro-Clobetasol Cream.
- - Product:
- .
- Technical: Patient DI/Lab Results Report, 2020-11-26
- Technical: Impax Viewer.
- Technical: Zeroviewer.
- Technical: NM Biliary HIDA Scan.
About: Dr. Stan Houston.
INDEX
https://www.ualberta.ca/medicine/about/people/sc-houston
LINK 2: https://www.ualberta.ca/public-health/
about/faculty-staff/adjunct-emeritus-faculty/houston
LINK 3: https://www.ualberta.ca/medicine/about/people/sc-houston
My over-arching interests are in the care of disadvantaged populations in Africa and other resource-limited settings as well as within our own community. My interest in public health and prevention of communicable diseases really arose from clinical experience with preventable illness.
I have a long standing interest in tuberculosis, in particular program development and implementation in low income countries as well as the interaction with HIV.
Favourite Quote: "The physician is the natural attorney of the poor." - Rudolph Virchow.
As medical program director of the Northern Alberta HIV program, I have an interest in local HIV epidemiology and treatment outcomes here in northern Alberta, but also in rural Uganda.
Finally, I am interested in the exciting progress against malaria, especially in Africa; specifically strategies for making reliable diagnosis and effective treatment accessible for children in rural Africa and developing a better understanding of non-malaria causes of fever and how to address them.
He received his MD from the University of Saskatchewan.
He has worked in primary care in northern Saskatchewan and rural Africa, and for 4 years in academic Medicine at the University of Zimbabwe. He also serves as consultant to Travellers Health Services, and the New Canadians Health Centre; and on the Board of Edmonton's needle exchange program. He initiated a course on the epidemiology & control of infectious diseases.
He is actively involved in international projects including Uganda.
He currently sits on the Council of the Alberta College of Physicians and on the board of the Parkland Institute.
His primary source of anxiety is current federal government policy in the area of refugee health, among other policies.
He has had training qualification in Family Medicine, Tropical Medicine, Internal Medicine Infectious Disease.
He has worked in primary care in northern Saskatchewan and rural Africa, and for 4 years in academic Medicine at the University of Zimbabwe.
He also serves as consultant to Travellers Health Services, and the New Canadians Health Centre; and on the Board of Edmonton's needle exchange program. He initiated a course on the epidemiology & control of infectious diseases. He is actively involved in international projects including Uganda.
He teaches in other disciplines, e.g. Parasitology and Pharmacy and has received awards for medical student, resident and Public Health graduate teaching.
He currently sits on the Council of the Alberta College of Physicians and on the board of the Parkland Institute.
He enjoys cycling, x-c skiing, running, theatre and reading and keeping up with the activities of his father, wife and 2 adult kids. His primary source of anxiety is current federal government policy in the area of refugee health, among other policies.
Degrees
MD, University of Saskatchewan, 1975
DTM&H, University of Liverpool, 1979
FRCPC, Canada, 1985
Awards
Adjunct faculty of the year, Department of Public Health Sciences, 2005
Small course teaching award, Public Health Students' Association, 2008
Leonard Tow Humanism in Medicine Award, Faculty of Medicine, 2008
Publications
Houston S, Wong T.
Tuberculosis and Human Immunodeficiency Virus.
In: Canadian Tuberculosis Standards 7th ed.
Ottawa: Health Canada and the Canadian Lung Association 2013.
Bright AT, Alenazi T, Shokoples S, Tarning J, Paganotti GM, White NJ, Houston S, Winzeler EA, Yanow SK.
Genetic analysis of primaquine tolerance in a patient with relapsing vivax malaria.
Emerg Infect Dis 2013;19(5):802-805.
Charles M, Patterson S, Asadi L and Houston S.
Persistent Hemolytic Anemia after Parenteral Therapy
with Artesunate for Severe Malaria in a Returning Canadian Traveler.
Emerg Infect Dis 2013 in press.
Tran BX, Ohinmaaa A, Mills S, Duong AT, Nguyen LT, Jacobs P, Houston S.
Multilevel predictors of confurrent opiod use during
methadone maintenance treatment among drug users with HIV/AIDS.
PLoS One 2012;7(12):e51569.
Kipp W, Konde-Lule J, Saunders LD, Alibhai A, Houston S, Rubaale T, Senthilselvan A, Okech-Ojony J.
Antiretroviral treatment for HIV in rural Uganda:
two-year treatment outcomes of a prospective health centre/community-based and hospital-based cohort.
PLoS One 2012;7(7):e40902.
Quotes: CBC News --- Posted: Jul 19, 2017
INDEX
Parasite worms its way into Alberta, infecting humans through dogs, coyotes.
https://www.cbc.ca/news/canada/edmonton/
parasite-tapeworm-university-alberta-coyotes-1.4212207
CBC News --- Posted: Jul 19, 2017
University of Alberta scientists are alerting the public to a potentially lethal tapeworm, which infects humans through the feces of coyotes and dogs.
'When we pet them and then touch our food or our mouths, we ingest the parasite's eggs'
Alberta biologists noticed a high infection rate of a tapeworm among Alberta coyote populations a few years ago, which is potentially lethal to humans.
Houston said the parasite, widely recognized in Europe, is rare in North America, but the potential consequences are life threatening.
Coyote tapeworm that infects dogs, humans spreading to cities
https://www.cbc.ca/news/technology/
coyote-tapeworm-that-infects-dogs-humans-spreading-to-cities-1.1175740
If left untreated, the parasite can kill its human host in 10 to 15 years, researchers said.
In most cases, the early presence of Echinococcus multilocularis has no symptoms.
"If the tapeworm goes unnoticed, it can spread to other parts of the body, much like how cancer invades and destroys organs," he added.
The infestation grows slowly, on average 14 cubic centimetres a year.
By the time it's found, it may be inoperable.
How parasite is transmitted
People can get the tapeworm from eating foods exposed to traces of canine
feces and should be especially vigilant in washing vegetables grown
close to the ground.
Houston said we should also be aware of microscopic traces of pet feces in our pets' hair.
"When we pet them and then touch our food or our mouths, we ingest the parasite's eggs," he said.
The parasite is largely harmless to dogs and coyotes only on rare occasions leading to illness or death.
Researchers recommend pet owners get their pets dewormed on a regular basis if they eat rodents or the feces of other dogs.
Standard dog deworming does not cover the tapeworm, but veterinarians can suggest the proper medication.
Houston said the parasite is an example of the ecological interaction between human and animal health.
"Most emerging infectious diseases come from animals and now here is another one right on our doorstep."
Quotes: CBC Radio --- Posted: Jun 07, 2019
INDEX
https://www.cbc.ca/radio/asithappens/as-it-happens-friday-edition-1.5166570/
brain-surgeons-went-looking-for-a-tumour-but-found-a-tapeworm-instead-1.5166571
N.Y. neurosurgeon Jonathan Rasouli says the unexpected parasite
looked like a quail egg from the grocery store
Written by Sheena Goodyear.
Interview with Dr. Jonathan Rasouli produced by Allie Jaynes.
This MRI scan of Rachel Palma' s brain revealed what appeared to be a brain tumour, but was, in fact, a baby tapeworm.
(Mount Sinai Health System)
The removal of the tiny parasite marked the conclusion of a more than year-long ordeal for Rachel Palma, a 42-year-old newlywed from Middletown, N.Y.
She first went to the doctor in January 2018 with a laundry list of neurological symptoms, she told the Washington Post.
She couldn' t sleep, and when she did, she had nightmares. She was hallucinating.
She had trouble talking. She kept dropping things. Her right hand and the right side of her face were numb.
An MRI scan revealed a lesion in the frontal left lobe of her brain.
That, combined with her symptoms, led doctors to conclude she had a brain tumour.
The only thing left to do was open up her skull and determine whether it was malignant or benign.
Neither the doctors nor Palma know how she got the parasite, which is called 'Taenia solium and is extremely uncommon in North America."
Some people get it by ingesting microscopic tapeworm eggs found in raw or undercooked pork, or unwashed fruits and vegetables from overseas. But Palma has never travelled outside the U.S.
People with adult tapeworms in their guts can also spread the parasite if the eggs are passed through their stool and they don' t properly wash their hands.
"These larvae or eggs can hatch and they can essentially migrate their way all throughout the body.
Sometimes they can develop into a large adult tapeworm in your colon," Rasouli said.
"And in other cases, which is frequently rare, they can migrate their way through the bloodstream and essentially try to develop into more adult forms all throughout the body� and because the brain has such a robust blood supply, one of the favourite places for that baby to go is the brain."
Quotes: CBC News -- Posted: Jul 25, 2019
INDEX
https://www.cbc.ca/news/canada/calgary/tapeworm-echinococcus-multilocularis
-alberta-klein-calgary-veterinarian-disease-coyotes-dogs-1.5224864
Tapeworm in coyotes that can cause fatal tumours in people 'has spread all over Alberta'
Dr. Alejandra Santa/Submitted by Albert Lee
The European strain of a tiny tapeworm that can make people seriously ill and even kill them is now common in wildlife throughout Alberta, Calgary researchers say.
A parasitic tapeworm called Echinococcus multilocularis is now very common in wildlife in Western Canada, scientists say.
The European strain of a tiny tapeworm that can make people seriously ill and even kill them is now common in wildlife throughout Alberta, Calgary researchers say.
The research was published in a letter in the New England Journal of Medicine.
The research, led by the University of Calgary's faculty of veterinary medicine, found that the parasitic tapeworm called Echinococcus multilocularis is now prevalent in Western Canada, after being first spotted there in 2012 and long common in Europe.
The first human case in Canada of a tumour-like disease caused by the tapeworm, human alveolar echinococcosis (AE), was diagnosed in 2013.
Dr. Claudia Klein, one of the study's authors, said her lab now has DNA samples from most of the 14 people in Canada who have been diagnosed to date with the potentially fatal parasite.
"If you're exposed to the tapeworm eggs, you can become infected with it," she said.
"The problem is, you won't really notice for years later that you're infected, and then your liver will be infiltrated by tumour-like lesions
from that tapeworm."
If the disease isn't discovered and treated, the mortality rate is 90 per cent, Klein said.
"So for humans, it's a very serious condition."
Klein said experts had assumed until recently that cases of AE were not showing up in North America because the strain of tapeworm on this
continent is not as virulent to people.
"But the story has really changed dramatically over the past five years," she said.
Klein says her lab is now finding, overwhelming, the European strain when researchers examine coyote feces and rodent livers.
"So, that was a very surprising finding," she said.
Klein collaborated on the research with Dr. Alessandro Massolo, who was teaching wildlife health ecology at the U of C and is
now at the University of Pisa in Italy, and with Dr. Kinga Kowalewska-Grochowska of the University of Alberta.
Strain arrives in dogs from Europe
It's believed the strain has been arriving in Canada in dogs that are brought over from Europe, and in foxes that were imported decades ago
for hunting.
Infected foxes and coyotes shed the tapeworm's eggs in their feces, which are eaten by small rodents such as deer mice and
voles.
In those animals, which are considered intermediate hosts, the eggs become larvae that form in large cysts. The cysts
eventually kill the rodent or render it vulnerable to prey. If those preying animals are coyotes or foxes, the larvae they ingest become
adult tapeworms, closing the circle.
Dogs can get the parasite in turn through contact with infected coyote or fox feces or by eating infected dead rodents.
The worms can be passed on to people on fruit, by handling contaminated soil or through an infected dog's fur, which can be
contaminated with worm eggs too small to see.
The human form of the disease develops slowly over several years and causes multiplying lesions in the body, usually in the liver.
"This evidence is the smoking gun that these AE cases are locally acquired, and they are caused by an invasive strain coming from Europe that has
spread all over Alberta," said co-author Dr. Alessandro Massolo.
"So, this European strain is known to be very virulent for people, and now is everywhere in wildlife and even in dogs. From a public health
perspective, to me is very relevant, because it has to change the way you assess the risk for this disease."
Klein says hunters and trappers are at an elevated risk of getting the disease from wild animals, while veterinarians can pick it up from dogs, which can also host the tapeworms.
'There's no need for panic'
"In dogs, we've found a low prevalence of that tapeworm," she said.
Pet owners can protect themselves by washing their hands after picking up their dog's waste.
"There's no need for panic or anything, just to be aware of it," she said.
But hunters and trappers should get their blood tested for the presence of antibodies, Klein said. "The earlier you find it the better."
The infection can be treated with anti-parasitic medication.
People with compromised immune systems are also more vulnerable to the disease
Quotes: Star Calgary -- Thu., July 25, 2019
INDEX
Dogs may be spreading fatal parasite found in Alberta coyotes, University of Calgary study finds
https://www.thestar.com/calgary/2019/07/25/dogs-and-cats-may-be-spreading-fatal-parasite
-found-in-alberta-coyotes-university-of-calgary-study-finds.html
By Amy Tucker --- Star Calgary
Thu., July 25, 2019
CALGARY�A potentially fatal parasite is now common in wildlife throughout Alberta and it can be spread to pets and their owners, new research has found.
A tiny, parasitic tapeworm known as Echinococcus multilocularis was detected in wildlife in Western Canada in 2012, according to a study led by the University of Calgary�s faculty of veterinary medicine that was released Thursday.
A year later, the first human case was diagnosed � called Alveolar echinococcosis � and appeared to be a tumour-like disease caused by the tapeworm.
Since 2016, there have been six more people diagnosed with the disease in Alberta.
The illness develops slowly over several years and causes tumour-like lesions in the body � often the liver � that multiply.
While strains of tapeworms vary, this one in particular may have originated in Europe and came to North America from dogs brought overseas, according to Claudia Klein, associate professor and co-lead researcher. The study was also led by Alessandro Massolo, adjunct professor of wildlife health ecology, and Kinga Kowalewska-Grochowska of the University of Alberta.
�Most people, when they hear �tapeworm� think about this long, white worm that lives in your intestine and sort of competes with you for your nutrients,� Klein said. �But this is a different species of tapeworm. It�s actually a tiny worm (that) you can barely see with your eyes, maybe just like a millimetre in size.�
The disease is spread through the tapeworm �life cycle,� Klein said.
Carnivores, such as foxes and coyotes can be hosts to the parasites and can live with no harmful impact from the tapeworms, which will live in their intestines. The parasites� eggs are then shed from the animal through its feces. But if a rodent comes into contact with the feces, it becomes infected. And when a fox or coyote, for example, eat the rodent, they become infected, too.
Quotes: CBC News --- Posted: Jan 23, 2020
INDEX
https://www.cbc.ca/news/canada/edmonton/
parasite-cassidy-armstrong-tapeworm-alberta-1.5436828
For this Alberta woman, the good news was she had contracted a rare, deadly parasite.
Ariel Fournier --- CBC News --- Posted: Jan 23, 2020
see the IMAGES in the original, or in the reformatted, article
Cassidy Armstrong discovered she had a 10-cm growth on her liver from a rare parasite that has emerged in Alberta.
Cassidy Armstrong went in for surgery last fall to remove what doctors thought was a tumour on her liver.
She had been diagnosed with a suspected rare cancer that, even with the surgery, would probably have left her with only a few years to live.
Instead, doctors found something even rarer: a grapefruit-sized mass caused by the eggs of a tapeworm.
A slow-spreading cyst from tapeworm eggs
The parasite lives as a tapeworm in coyotes, foxes and, increasingly, domestic dogs.
The tapeworm's eggs are spread to other animals, such as rodents, from the feces of infected animals.
When a person accidentally swallows the microscopic eggs, the infection can lead to cyst-like lesions on the liver.
But it will only cause minimal symptoms until the growths reach a significant size.
Echinococcus multilocularis is a rare parasite that forms as cysts on the liver in humans when they accidentally eat microscopic tapeworm eggs spread through canine feces.
(Centre for Disease Control website)
The tapeworm had likely been growing inside Armstrong, 36, for more than a decade.
"It was almost a Christmas miracle," she said.
"It could have been a lot worse."
Armstrong had worked physically demanding jobs -- she'd been a motorcycle mechanic in Edmonton before moving to Banff last year
to work as a stage carpenter -- and was in good health, though occasionally noticed she was fatigued.
About two years ago, she felt tenderness in her ribs.
X-rays didn't find anything, she said, and eventually the pain subsided.
While in Banff, the pain in her side returned and became almost constant.
It was accompanied by a new pain in her shoulder.
-
As It Happens: https://www.cbc.ca/radio/asithappens/as-it-happens-friday-edition-1.5166570/
brain-surgeons-went-looking-for-a-tumour-but-found-a-tapeworm-instead-1.5166571
She worried she had gallstones and insisted on an ultrasound.
That's when the mass was discovered, she said, leading to the cancer diagnosis and grim news that surgery wouldn't guarantee her more than a few more years.
"I would have lived maybe another two to five years.
There were a lot of things going through my mind," she said.
"Mainly, what's the point?"
Growing number of cases in Alberta
Her cancer surgery was the equivalent of an open-heart operation.
Surgeons removed her gallbladder, 65 per cent of her liver and cut several nodes off her lungs, in addition to scraping the cyst off her diaphragm. She has a 14-inch, L-shaped scar on her chest that is still not completely closed, two months after surgery.
Armstrong's parasitic clump is one of the largest physicians have seen in Alberta. And they've seen a few.
"We're definitely the hot spot,"
said Dr. Stan Houston, an infectious disease specialist at the University of Alberta.
Dr. Stan Houston is one of Canada's leading experts in Echinococcus multilocularis, a parasite spread to humans through tapeworm eggs.
(Ariel Fournier/CBC)
To date, there have been 15 cases of Echinococcus multilocularis in Alberta.
When Armstrong's case is scientifically confirmed, she will be number 16, he said.
It's believed the strain has been arriving in Canada in dogs brought over from Europe and in foxes imported decades ago for hunting.
It has existed in Europe for around 150 years.
There are about 1,800 human cases every year, the majority of which are found in China and Tibet.
A 2012 study found that the parasite was well-established in Alberta's wild animal population, with about one-quarter of the province's coyote population infected with the tapeworm.
The first Canadian human case was diagnosed in 2013.
"[Before the last decade] we never had people with this disease in all of North America," Houston said.
"In the last six years, we've had 15 definitely proven cases, just in Alberta."
Since 2014, Canadian researchers have warned that the parasite could easily be misdiagnosed by physicians as another liver disease or ailment.
"About half our cases were found by accident," Houston said.
In those cases, imaging revealed an abnormal growth in the liver.
Medication not available in Canada
There's no guaranteed cure for Echinococcus multilocularis.
Infected patients must take a parasite medication for the rest of their lives to prevent the tapeworm eggs from causing further growths.
A drug called albendazole, normally used to treat other tropical parasites, can act as a preventative treatment. While it is widely available in Africa, Europe and Asia, the drug company hasn't applied to Health Canada to access the Canadian market.
Houston said he applies for special access to the drug every 6 months on behalf of his patients.
A spokesperson for Health Canada said there are clinical trials in Canada that may lead to approval in the future.
How to avoid infection
Armstrong doesn't know how she was infected, but suspects it could have come from her work fixing farm equipment or from produce purchased at farmer's markets.
Houston said most patients in Alberta were dog owners, but Armstrong hasn't had pets since she was a kid.
Houston's main advice for prevention is meticulous hand-washing, particularly if you have dogs at home. Regularly de-worming your dog can be helpful as well.
"We're hoping to learn more about the ecology of this disease in Alberta so we can give more precise advice," he said. ...
About: Echinococcus multilocularis.
INDEX
https://en.wikipedia.org/wiki/Echinococcus_multilocularis
23 January 2020
The parasite is commonly maintained in a wildlife life cycle involving two mammalian hosts.
Wild canids, dogs, and less commonly cats act as definitive hosts, harbouring the adult stage of the tape worm.
Ingestion of a rodent containing alveolar hydatid cysts by a wild canid can result in a heavy infestation of tapeworms.
Signs and symptoms
Human alveolar echinococcosis is characterized by a lengthy incubation period of 5 to 15 years in immunocompetent individuals. The progression of disease is potentiated in immunocompromised patients. Following the ingestion of the eggs of E. multilocularis, the metacestode (larval) stage of the parasite typically embeds in the liver. As the disease progresses, the larval stage proliferates exogenously within the tissue, behaving similar to hepatic neoplasia. Patients with human alveolar echinococcosis typically present with
- headache,
- nausea,
- vomiting,
- abdominal pain.
- Jaundice is rare, but
- hepatomegaly is a common physical finding.
Morphology
The adult parasite is a small tapeworm that is 3- 6mm long, and lives in the small intestine of canines.
The segmented worm contains a scolex with suckers and hooks that enable attachment to the mucosal wall, since tapeworms do not have a digestive tract. A short neck connects the head to three proglottids, the body segment of the worm which contains the eggs to be excreted in the feces.
Diagnosis
Serological and imaging tests are commonly used to diagnose this disease.
Since the serological tests for alveolar echinococcosis only indicate exposure to the parasite and not ongoing infection, visualization of the parasitic mass is required to confirm the diagnosis. Frequently used serological tests include antibody tests, ELISA and indirect hemaglutination (IHA). Also, an intradermal allergic reaction test (Casoni test) has also been used to diagnose patients. Imaging tests include: X-rays, CT scans, MRI, and ultrasound.
Disease staging
Alveolar echinococcosis (AE) is a highly lethal helminthic disease in humans, caused by the larval form of the parasitic tapeworm E. multilocularis. The disease represents a serious public threat in China, Siberia, and central Europe. However, since the 1990s, the prevalence of the disease seems to be increasing in Europe, not only in the historically endemic areas but its neighboring regions. AE primarily affects the liver by inducing a hepatic disorder similar to liver cancer, therefore becoming extremely dangerous and difficult to diagnose. If the infection metastasizes, it may spread to any other organ and could be lethal if not treated. The most common treatment for AE is to surgically remove the parasite. Since it is difficult and not always possible to remove the entire parasite, medicine such as Albendazole is utilized to keep the cyst from growing back.
Article: Echinococcus multilocularis Infection, Southern Ontario, Canada.
INDEX
https://wwwnc.cdc.gov/eid/article/25/2/18-0299_article
Jonathon D. KotwaComments to Author , Mats Isaksson, Claire M. Jardine, G. Douglas Campbell,
Olaf Berke, David L. Pearl, Nicola J. Mercer, Eva Osterman-Lind, and Andrew S. Peregrine
Volume 25, Number 2 -- February 2019
...
We measured an infection prevalence of 34% (95% CI 28%�40%) among wild canids within the southern Ontario hotspot.
Consequently, a question of public health importance is to what extent the human population in southern Ontario is at risk for human AE. Across the endemic countries in Europe, where the prevalence of E. multilocularis infection in wild canids ranges from <1% to >50%, human AE is rare; the overall average annual incidence in these countries ranges from 0.03 to 0.3 cases/100,000 residents. However, substantial variation in risk exists across regions.
For example, in areas with consistently high prevalence in wild canids (i.e., 35%�65% prevalence), the annual incidence of human AE can be as high as 8.1 cases/100,000 residents, which is similar to the prevalence estimates among wild canids in the southern Ontario hotspot that we describe. Furthermore, the location of the infection cluster encompasses multiple urban areas with human population densities of up to 1,700 residents/km2. Therefore, transmission of E. multilocularis tapeworms should be considered a public health risk.
In areas endemic for E. multilocularis tapeworms, dog ownership has been associated with increased risk for human AE.
Dog ownership might entail various human and dog behaviors that might lead to an increased risk for human infection with E. multilocularis tapeworms. These behaviors include
leaving dogs outside unattended,
walking dogs without a leash,
allowing dogs to consume rodents, and
inconsistent deworming of dogs.
As such, monthly treatment with praziquantel is recommended for dogs that consume rodents in AE-endemic areas to prevent patent intestinal infections and therefore mitigate the risk for transmission to humans. The same is also recommended for dogs with hepatic AE because such dogs might also have concurrent intestinal infections. Thus, even in instances of canine hepatic AE, a follow-up investigation of possible exposure to E. multilocularis tapeworms for in-contact humans is warranted .
As of January 1, 2018, E. multilocularis infection was designated a reportable disease in animals in Ontario.
Veterinarians and diagnostic laboratories are required to report animal cases directly to their local PHUs to minimize potential risks to human and public health. Furthermore, as of May 1, 2018, E. multilocularis infection in humans was designated a disease of public health importance (i.e., a disease that must be reported) in Ontario.
Although human AE was not reportable before 2018, data from the Canadian Institute for Health Information indicate that >3 cases of human AE have been diagnosed in Ontario since 2014; however, these data do not include information regarding patient travel or exposure histories. Therefore, whether these cases were locally acquired is unknown.
Designating E. multilocularis infection as reportable in humans and animals is potentially important because, in AE-endemic areas (i.e., Europe), a large proportion of the economic burden associated with human AE is attributable to patients typically being diagnosed in the late stages of the disease, requiring lifelong chemotherapy and occasionally interventional procedures (e.g., percutaneous biliary and centroparasitic abscess drainage). Therefore, the ability to anticipate E. multilocularis exposure and to diagnose early-stage human AE is essential to reduce the need for long-term treatment, thereby minimizing the economic burden associated with the disease.
A limitation of having the infection reportable only in humans is that, given the long clinical incubation period of AE in humans, other persons potentially at risk would likely have been infected years earlier. Thus, in areas where E. multilocularis infection is endemic, a One Health surveillance approach that also requires mandatory reporting of E. multilocularis infection in animals to public health authorities could improve rates of prompt investigation of suspected exposure in persons and lead to earlier diagnosis.
Article: Cutaneous Disease as the First Manifestation of Cystic Echinococcosis.
INDEX
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4973166/
Virginia Velasco-Tirado, Manuela Yuste-Chaves, and Moncef Belhassen-Garc�a
Am J Trop Med Hyg. 2016 Aug 3; 95(2): 257�259.
A 61-year-old man from a rural area (Salamanca, Spain), who had contact with dogs, was admitted with generalized itching for 4 years. He was treated with oral antihistamines. A physical examination revealed greyish hyperpigmentation and severe lichenification and infiltration on the face, without mucosal pigmentation. His trunk and limbs showed xerosis, erythematous scaly skin areas with lichenification and hyperpigmentation.
Increased levels of IgE of 2,864 UI/L (0�114 IU/L), but no eosinophilia, were detected.
Skin biopsy revealed perivascular spongiotic dermatitis with eosinophilic infiltrate, congruent with eczema (Figure 2 ). Allergic and photoallergic contact dermatitis and aeroallergen sensitization were ruled out.
Bronchial hyperresponsiveness was determined and the patient was treated with salbutamol inhalation.
After a diagnosis of generalized eczema, he was managed with topical propionate of clobetasol and topical tacrolimus, oral ebastine, and oral prednisone in a tapering regimen during flares.
Skin lesions worsened with bronchial reactivity 4 years later.
IgE > 5,000 UI/L and eosinophilia of 900/�L (7.19%) were detected.
Chest X-ray was normal.
Antibodies against hepatitis B virus, hepatitis C virus, syphilis, Trichinella sp., Toxoplasma gondii, Strongyloides sp., Fasciola hepatica, Taenia solium, and parasites in stool (three serial samples) were negative.
IgG results for hydatic disease were repeatedly negative, but specific Echinococcus granulosus IgE was detected (3.13 kUA/L) (negative < 0.35 kUA/L, ImmunoCAP system, Phadia, Uppsala, Sweden).
Abdominal computerized tomography (CT) showed three focal lesions that were consistent with hepatic hydatid cysts: the first cyst was localized in segment I of 24 � 21 � 18 cm (stage cystic echinococcosis [CE] 5), the second cyst in segment II of 48 � 31 � 36 cm (stage CE3), and the third cyst in segment VII of 45 � 34 � 34 cm (stage CE3) (Figure 3 ).
Albendazole (400 mg twice a day) and praziquantel (1,200 mg twice a day) were administered and surgery was subsequently performed. Removal of cysts in segment I, II, and VII was done. Histopathological examination confirmed infection by E. granulosus.
Treatment with only albendazole was continued because of digestive intolerance from praziquantel. The patient improved symptomatically and with regard to the skin lesions (Figure 4 ). All treatments (topical, oral, and inhaled) were stopped after 18 months.
In dermatology, increased levels of IgE and eosinophilia are commonly related to atopy, but other entities with skin manifestations, mainly neoplasms and infectious diseases, should also be considered.
CE is a chronic, complex, and neglected zoonotic disease, and it remains an important health problem in many areas of the world. In humans, it may result in a wide spectrum of clinical manifestations, ranging from asymptomatic infection to severe and even fatal disease. CE typically grows slowly and may long remain clinically silent.
Common serodiagnotis techniques may produce a high percentage of false-negative results, and thus CE diagnosis can be difficult. Echinococcus granulosus infection may produce different cutaneous manifestations, some of which are due to mechanical complication, such as skin fistulae, and others are due to anaphylactoid reactions, such as acute or chronic urticaria and flushing.
It is assumed that these former symptoms may be caused by a partial rupture of the cyst with microscopic drainage.
We propose that this continuous antigenic trigger and repeated scratching could potentially result in clinical manifestations in our patient, which were resolved using antiparasitic treatment. We have not found any previously described association between the skin alterations in our patient and hydatid disease.
In conclusion, we highlight that skin manifestations may be a clue in the diagnosis of potentially severe infectious diseases, and we should include CE in the differential diagnosis of generalized eczema.
Footnotes
Authors' addresses:
Virginia Velasco-Tirado and Manuela Yuste-Chaves,
Service of Dermatology, University Hospital of Salamanca,
Salamanca, Spain --- E-mails: se.oohay@alevriv and moc.liamtoh@etsuyaleunam.
Moncef Belhassen-Garc�a, Service of Internal Medicine,
Unit of Infectious Diseases, University Hospital of Salamanca,
Salamanca, Spain --- E-mail: moc.liamtoh@nessahlebm.
Article: Superinfection of a Dead Hepatic Echinococcal Cyst
with a Cutaneous Fistulization.
INDEX
https://www.hindawi.com/journals/crira/2017/9393462/
Giuseppe Cicero , Alfredo Blandino , Giorgio Ascenti, Tommaso D�Angelo , Luciano Frosina,
Carmela Visalli, Ignazio Salamone, Maria Adele Marino, Marco Cavallaro, and Silvio Mazziotti
Case Reports in Radiology --- Volume 2017 |Article ID 9393462 | 5 pages
Additional LINK: https://doi.org/10.1155/2017/9393462
IMAGES noted can be observed in the original document at the above LINKS.
1. Introduction
Cystic echinococcosis (CE), also known as �hydatid disease� (HD), is a zoonotic infection caused by the larval stage of Echinococcus granulosus, which accidentally infects humans through the orofecal route.
Although previously endemic in Africa, South America, and Eurasia, the disease is nowadays worldwide spread due to the increased migratory flows.
Because of the intestinal absorption, the main organ affected is the liver (70% of cases), where the hydatid cyst can develop.
In most cases, the disease is asymptomatic and the typical cystic lesion can be depicted as an incidentaloma while performing imaging examinations.
Otherwise symptoms may be aspecific (weight loss, anemia, fatigue, etc.) or related to complications, such as rupture of the cysts (spontaneous, traumatic, or iatrogenic), secondary infection, and cholangitis.
The final diagnosis is reached matching patient�s clinical history, specific serologic tests, and imaging evaluation, helpful in providing a complete clinical picture.
According to the radiological findings, several classifications have been proposed, all in agreement in defining thick-calcified-wall cysts as inactive or dead.
We show an unusual case of superinfection of a dead calcified hydatid cyst (WHO-type CE5) with an even rarer skin fistulization passing through a subcutaneous-abdominal abscess involving the right iliac muscle.
2. Case Report
A 68-year-old male patient suffering from chronic renal and heart failure and alcohol-related cirrhosis was admitted to our hospital with fever, abdominal pain, and a right-flank fistula, draining a huge quantity of purulent secretion.
He had also a known history of CE with a calcified cysts of the liver, incidentally discovered a few years before at a chest X-ray in our department and confirmed at unenhanced CT-scan.
Laboratory tests showed a neutrophilic leukocytosis (WBC 11300; N: 84%) and an electrolyte imbalance with severe hyponatremia.
An ultrasound (US) examination of the abdomen was immediately performed, showing the presence of a subcutaneous abscess.
To better evaluate the size and depth of the abscess he underwent an MR examination performed in our department using a 1.5 T MR Philips Gyroscan Intera (Philips Medical System, Best, Netherlands) and phased-array abdominal coils.
Different pulse sequences were applied:
2D axial and coronal T2-weighted turbo spin echo (TSE) sequences,
2D axial echo-planar imaging (EPI) sequence at different values (: 0, 500, 800?s/mm2), and
2D T1-weighted axial dual fast-field-echo (FFE) breath-hold sequence.
Intravenous injection of contrast medium was avoided due to the chronic renal failure of the patient.
MRI confirmed the presence of an inhomogeneous fluid collection with irregular peripheral walls, indicative of abscess, extending from the subcutaneous tissues of the posterior right abdominal flank into the abdominal cavity, through the right iliac muscle. The abscess showed a middle-low T2 hyperintensity of the content while DWI study revealed diffusion restriction of the lesion (Figure 2).
A long narrow fistula connecting the abscess with the hepatic hydatid cyst was also found.
In order to better assess the route of that fistulous tract, a CT-fistulography was obtained catheterizing the external opening of the fistula with a thin cannula and injecting a water-soluble iodine contrast medium. The exam showed a progressive contrast filling of the abscess and the abdominal fistula (Figure 3), ascending till the calcified hydatid cyst of the liver.
The drainage culture test showed the presence of Pseudomonas aeruginosa and Klebsiella oxytoca, without any Echinococcus.
Afterwards, the patient underwent an antibiotic therapy with percutaneous drainage of the cutaneous-abdominal abscess. After the complete resolution of the abscess, a surgical cystectomy was performed.
3. Discussion
Echinococcosis is a worldwide zoonosis, caused by Cestode parasites, commonly known as small tapeworms of carnivorous animals, that can infect humans, as intermediate hosts, through the orofecal route.
The liver is the most common organ involved (75% cases of HD), followed by the lungs (15%).
Although the course of the liver hydatid disease is usually asymptomatic, complicated forms are not rare, occurring in 30�60% of the patients.
The main complications include traumatic or idiopathic rupture of the cysts into the biliary tract, which is the most frequent, or into peritoneum, skin, digestive tract, or thorax, due to a transdiaphragmatic involvement.
Large and superficial hepatic cysts are considered to be the most susceptible to break.
�Mass-effect� of large lesions may also cause vascular complications, such as
Budd-Chiari and vena-cava syndromes, and
biliary obstruction that may lead to cholestatic jaundice, cholangitis, biliary colic, and fever.
Suppuration of the cyst is caused by a cystobiliary communication and it is not a rare complication, with an occurrence of 5�40%.
However, although the association between calcified hydatid cysts and suppuration is well known, to our knowledge, there are not a clear percentage of occurrence and no imaging descriptions in cysts with an egg-shell thick calcified wall that is usually considered a feature of inactivity.
Certainly, imaging techniques play a pivotal role in a comprehensive evaluation of hydatid disease.
Though abdominal ultrasonography is considered the gold standard in identifying and characterizing the cysts, CT and MRI have reached an increasing importance over the years.
In fact, while CT-scan has a good sensitivity and specificity in the evaluation of hepatic HD, especially in depicting wall calcifications, MRI is nowadays considered the best imaging investigation in differentiating the fluid content of the cyst from other components and in depicting vascular or biliary tree involvement and extrahepatic complications.
On the basis of imaging findings, several classifications have been proposed in typifying echinococcal cysts, but only few of them achieved a large consensus.
Through a sonographic evaluation, Gharbi et al. proposed a subdivision of the hydatid cysts into 5 types:
- a simple fluid collection (type I),
- a fluid collection with split wall (type II),
- a fluid collection with septa (type III),
- a cyst with heterogeneous echo patterns (type IV), and
- a cyst with reflecting thick walls (type V).
In order to establish a simpler and standardised classification, also able to reflect the stages of the disease and the related treatment, a new one was introduced in 2003 by the Informal Working Group on Echinococcosis (IWGE-WHO). Still relayed on ultrasound examination, this classification recognizes 6 categories of hydatid cysts:
- CL, a simple cyst with anechoic content and not clearly visible wall, suspicious for an early stage of EC;
- CE1, a cyst with visible wall containing an inhomogeneous fluid due to the presence of hydatid sand;
- CE2, a multiseptate cyst with daughter cysts inside, with variable appearance (�rosetta-like,� �wheel-like,� or �honeycomb-like� structure);
- CE3, characterized by anechoic content with detached membranes within (3a) or daughter vesicle inside solid-echoic areas (3b), related to degenerated daughter cysts;
- CE4, hypoechoic or inhomogeneous content without daughter cysts;
- CE5, with thick calcified wall with a cone shadow.
Moreover, these categories were grouped on the basis of their physiopathological behaviour into 3 types:
- active (CL, CE1, CE2),
- transitional (CE3), and
- inactive (CE4, CE5).
However, the inclusion of CE4 type in the inactive group has raised some doubts, due to the presence of fertile liquid inside the vesicles; this implies a consequent �watch and wait� clinical approach.
Another widely used brief classification, suggested by Precetti et al. , divides the cysts in 4 types on the basis of the imaging findings:
- simple cyst with noninternal architecture (type I);
- cyst with daughter cysts and matrix (type II);
- calcified cyst (type III);
- complicated cyst (type IV).
Nowadays, 3 different options are available while treating uncomplicated CE: surgery, PAIR, and chemotherapy. CE4 and CE5 types are generally excluded from any kind of therapy and a �watch and wait� strategy is actually recommended.
Surgical treatment consists of different approaches, from the conservative (simple-closure tube drainage or marsupialization) to the radical ones (cystectomy or hepatic resections). Despite its invasiveness, it still remains the first choice in the treatment of large CE2�CE3b or complicated EC.
PAIR (an acronym that stands for �puncture, aspiration, injection, reaspiration�) technique has gained momentum during the last two decades, due to its lower invasiveness. It consists in a US-guided needle aspiration of half volume of an EC followed by the injection of a hypertonic saline solution or ethanol and it is mainly indicated for CE1 and CE3a cysts bigger than 5 cm. The main limitations of PAIR include biliary communication, infection of the cyst cavity, and, although very rare, anaphylactic reactions.
On the other hand, chemotherapy consists in the administration of mebendazole (MBZ) or albendazole (ABZ) and it can be combined as an adjuvant to surgery or PAIR.
The treatment of CE2 and CE3b cysts has been discussed over the years, due to their typical trend to relapse.
Although some works suggest to choose an expectant management, in particular for C3b types, Akhan et al. have recently achieved better results in terms of decreased complications and lower recurrence, using a �modified catheterization� PAIR technique that also includes the removal of the solid components of the cyst.
As a matter of fact, in our case, the patient was affected by a hepatic hydatid cyst, previously demonstrated in a CT-scan performed in our department, completely surrounded by a thickened calcified wall.
Nevertheless, at the patient�s latest hospitalization, a very serious superinfection of that cyst was found.
In particular, sonography and MRI showed the presence of a large abscessual collection located in the subcutaneous tissues of the posterior right flank and extending into the abdominal cavity through the right iliac muscle.
Moreover, the abscess was in communication superiorly with the hydatid cyst of the liver, through a thin intra-abdominal fistula and inferolaterally to the skin surface.
In order to completely assess the length, the size, and the orientation of that fistula, a CT- fistulography was obtained, which clearly enhanced the whole route.
A cutaneous involvement with a spontaneous skin fistulization is considered a very rare complication of liver hydatidosis and only a few cases have been reported.
Skin fistulization generally occurs at the same anatomic level of the hepatic cyst, as a result of some pathophysiological steps: protrusion of the cyst into the innermost muscular layer of the abdominal wall, penetration into the muscular tissue, subcutaneous rupture, and/or skin fistula formation.
In our case, a progressive cystic adhesion to the abdominal wall did not occur and the external opening was very far from the hepatic hydatid cyst, considering that the fistula was located in the lateral abdominal cavity and connected downwards to the subcutaneous-abdominal abscess which involved the right iliac muscle.
To our knowledge, the involvement of the iliac muscle has never been reported in the literature up to now.
In conclusion, we showed an unusual case of superinfection of an inactive calcified hydatid cyst with an even rarer abdominal-cutaneous fistulization passing through a subcutaneous-abdominal abscess involving the right iliac muscle.
Furthermore, it demonstrates the usefulness of MRI not only in
- identifying the cystic content,
- the extension of the disease, and
- the related complications, but also in
- identifying the thin fistulous tract
in order to allow a better treatment planning.
Article: Echinococcus multilocularis:
An Emerging Pathogen in Hungary and Central Eastern Europe?
INDEX
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2958538/
Emerg Infect Dis. 2003 Mar; 9(3): 384�386.
Tam�s Sr�ter, Zolt�n Sz�ll, Zsuzsa Egyed, and Istv�n Varga
... According to some authors, researchers cannot confirm whether E. multilocularis is spreading from historically known E. multilocularis�endemic foci (eastern France, southern Germany, northern Switzerland, and western Austria) to new regions, or whether the Central European E. multilocularis�endemic area is connected with the E. multilocularis�endemic area in Asia, and the tiny worms previously escaped the attention of parasitologists. Our findings may suggest that the parasite�s range has recently expanded, rather than the first identification of formerly unknown E. multilocularis�endemic areas.
The parasite was not identified previously in either Red Foxes or wild rodents in Hungary, despite the extensive studies conducted by Murai, M�sz�ros, Gub�nyi, and other parasitologists of the Natural History Museum, Budapest. Moreover, human cases have never been reported in Hungary. The photograph and the description of macroscopic lesions (two fist-sized, undulating cysts) in the only presumed report of alveolar echinococcosis written by two surgeons clearly indicate that the case was indeed cystic echinococcosis.
The appearance of E. multilocularis in Hungary might be explained by changes in the size of the Red Fox population in central and Central Eastern Europe. From the 1970s, a continuous increase in the size of the Red Fox population was observed in Switzerland and Germany, probably as a consequence of the initiation of the antirabies vaccination programs. The larger population led to a continuous migration of young foxes from territories with high population density toward those with lower density, i.e., partly eastward. This migration might have resulted in the appearance of foxes infected with E. multilocularis and the establishment of small disease-endemic foci in Poland and the Czech Republic.
After the political changes of 1990, considerable changes in land use were observed in the former communist countries because of the disintegration of large state farms. The probable consequences of these changes, the decrease of annual hunting index resulting from a decrease in the price of fox fur, and the initiation of antirabies vaccination of foxes in Central Eastern European countries (Poland, the Czech Republic, the Slovak Republic, and Hungary), caused a corresponding increase in the fox population size, and probably the coincidental increase of E. multilocularis population and prevalence and the expansion of E. multilocularis�endemic regions. A similar positive correlation between the population size of foxes and the prevalence of the parasite was also observed in Switzerland and Germany.
In the historically known E. multilocularis�endemic region, almost 400 patients are currently under continuous therapy, and the annual incidence of human alveolar echinococcosis has not varied markedly in the past few decades. In contrast with the stable epidemiologic situation in that region, the first 16 sufficiently documented and undoubtedly confirmed autochthonous human infections have been reported in Central Eastern European countries only from the late 1990s. Based on Central European annual incidence data (approximately 0.1�0.3/100,000 population) and the similar overall prevalence of infection in foxes in Central and Central Eastern European countries, hundreds of cases would have been expected in the past few decades. The tiny worms may have escaped the attention of Central Eastern European parasitologists earlier. However, failing to recognize the characteristic and extensive lesions in humans in the past is unlikely.
Data from the Netherlands, Italy, Hokkaido Island and the surrounding islands of Japan, and North America provide clear evidence for the spreading and emergence of E. multilocularis infection. In the past, E. multilocularis has spread from the tundra zone of Northern Canada to the central regions of the continental United States and from a small focus to the entire Hokkaido Island. Based on the above data, a similar spreading and emergence are likely being observed in Central Eastern European countries.
As a result of their increasing population, foxes are inhabiting urban areas in several European countries, including Hungary. The appearance of foxes in a synanthropic environment may result in the infection of domesticated dogs and cats and may increase the risk for human infections in E. multilocularis�endemic areas. Thus, knowing that E. multilocularis is likely to continue to spread, one can predict that human alveolar echinococcosis will become an emerging infectious disease in Central Eastern European countries in a few years as has already occurred in some other European countries, Hokkaido Island of Japan, Canada, and the United States.
Article: Alveolar echinococcosis (AE), USA CDC.
INDEX
https://www.cdc.gov/parasites/echinococcosis/gen_info/ae-faqs.html
Page last reviewed: December 12, 2012
LINK 2: https://www.cdc.gov/parasites/echinococcosis/index.html
Page last reviewed: December 12, 2012
LINK 3: https://www.cdc.gov/parasites/echinococcosis/health_professionals/index.html
Page last reviewed: August 28, 2019
Alveolar echinococcosis (AE) disease is caused by infection with the larval stage of Echinococcus multilocularis,
a ~1-4 millimeter long tapeworm
found in foxes, coyotes, and dogs (definitive hosts).
Small rodents are intermediate hosts for E. multilocularis.
Although cases of AE in animals in endemic areas are relatively common, human cases are rare. AE ... causing parasitic tumors that can form in the liver, lungs, brain, and other organs. If left untreated, AE can be fatal.
How do people get alveolar echinococcosis (AE)?
People who accidentally swallow the eggs of the Echinococcus multilocularis tapeworm are at risk for infection.
People at high risk include trappers, hunters, veterinarians, or others who have contact with wild foxes, or coyotes, or their stool, or household dogs and cats that have the opportunity to eat wild rodents infected with AE. Humans can be exposed to these eggs by �hand-to-mouth� transfer or contamination.
By directly ingesting food items contaminated with stool from foxes or coyotes.
This might include grass, herbs, greens, or berries gathered from fields.
By petting or handling household dogs or cats infected with the Echinococcus multilocularis tapeworm.
These pets may shed the tapeworm eggs in their stool, and their fur may be contaminated.
Some dogs �scent roll� in foreign material (such as wild animal feces) and may become contaminated this way.
Where is alveolar echinococcosis (AE) found?
AE is found worldwide, mostly in northern latitudes.
Cases have been reported in central Europe, Russia, China, Central Asia, Japan, and North America.
In North America Echinococcus multilocularis is found primarily in the north central region from eastern Montana to central Ohio, as well as Alaska and Canada. Rare human cases have been reported in Alaska, the province of Manitoba, and Minnesota.
Prevalence among wild foxes and coyotes can be high, and may reach over 50% in some areas; however, even in these areas, transmission to humans has been low.
Alveolar Echinococcosis
The primary infection of alveolar echinococcosis is in the liver, usually the right lobe, but direct extension to contiguous organs, as well as hematogenous metastases to the lungs and brain is not uncommon. Alveolar echinococcosis is inhibited by the host from completing its development and remains in the proliferative stage indefinitely. The larval mass resembles a malignancy in appearance and behavior.
In chronic alveolar hydatid infections, the lesion consists of a central necrotic cavity filled with a white amorphous material that is covered with a thin peripheral layer of dense fibrous tissue. Host tissue is directly invaded by extension of the budding and proliferating cyst wall, causing a pressure necrosis of surrounding host tissue. A vigorous inflammatory and fibrous tissue reaction usually surrounds the larval mass. Diagnosis is often delayed until an advanced and inoperable stage; mortality rates have traditionally been high, ....
What are the symptoms of alveolar echinococcosis (AE)?
AE is caused by tumor-like or cyst-like tapeworm larvae growing in the body.
AE usually involves the liver, but can spread to other organs of the body.
Because the cysts are slow-growing, infection with AE may not produce any symptoms for many years.
Pain or discomfort in the upper abdominal region, weakness, and weight loss may occur as a result of the growing cysts.
Symptoms may mimic those of liver cancer and cirrhosis of the liver.
Persons with cystic echinococcosis often remain asymptomatic until hydatid cysts containing the larval parasites grow large enough to cause discomfort, pain, nausea, and vomiting. The cysts grow over the course of several years before reaching maturity and the rate at which symptoms appear typically depends on the location of the cyst. The cysts are mainly found in the liver and lungs but can also appear in the spleen, kidneys, heart, bone, and central nervous system, including the brain and eyes. Cyst rupture is most frequently caused by trauma and may cause mild to severe anaphylactic reactions, even death, as a result of the release of cystic fluid.
Alveolar echinococcosis (AE) is characterized by parasitic tumors in the liver and may spread to other organs including the lungs and brain. In humans, the larval forms of E. multilocularis do not fully mature into cysts but cause vesicles that invade and destroy surrounding tissues and cause discomfort or pain, weight loss, and malaise. AE can cause liver failure and death because of the spread into nearby tissues and, rarely, the brain. AE is a dangerous disease resulting in
a mortality rate between 50% and 75%, especially because most affected people live in remote locations and have poor health care.
What should I do if I think I have alveolar echinococcosis (AE)?
See your health care provider if you think you may have alveolar echinococcosis (AE).
Diagnosis of AE can be made by a blood test that looks for the presence of antibodies to Echinococcus multilocularis.
Radiography permits the detection of hydatid cysts in the lungs; however, in other organ sites,
calcification is necessary for visualization.
Ultrasonography has been widely used for screening, clinical diagnosis, and monitoring of treatment of liver and intra-abdominal cysts. Cyst viability cannot be reliably determined with radiography or parasite antigen detection; calcification can be present in all stages of cysts.
Alveolar echinococcosis closely mimics hepatic carcinoma or cirrhosis and is more commonly diagnosed in people of an advanced age. Plain radiographs show hepatomegaly and characteristic scattered areas of radiolucency outlined by
calcific rings 2 to 4 mm in diameter. The usual CT image of E. multilocularis infection is that of indistinct solid tumors with central necrotic areas and perinecrotic plaque-like calcifications.
How is alveolar echinococcosis (AE) treated?
Surgery is the most common form of treatment for AE, although removal of the entire parasite mass is not always possible.
After surgery, medication may be necessary to keep the cyst from growing back.
... surgery remains the most effective treatment to remove the cyst and can lead to a complete cure.
Some cysts are not causing any symptoms and are inactive; those cysts often go away without any treatment.
The treatment of alveolar echinococcosis is more difficult than cystic echinococcosis and usually requires
radical surgery, long-term chemotherapy, or both.
Alveolar echinococcosis requires chemotherapy with or without surgery; radical surgery is the preferred approach in suitable cases. Effective treatment involves benzimidazoles administered continuously for at least 2 years and patient monitoring for 10 years or more since recurrence is possible. This has inhibited progression of alveolar echinococcosis and reduced lesion size in approximately half of treated cases. Intermittent treatment with albendazole is not recommended.
Can alveolar echinococcosis (AE) be prevented?
If you live in an area where Echinococcus multilocularis is found in rodents and wild canines, take the following precautions to avoid infection:
-
Don�t touch a fox, coyote, or other wild canine, dead or alive, unless you are wearing gloves.
Hunters and trappers should use plastic gloves to avoid exposure.
- Don�t keep wild animals, especially wild canines, as pets or encourage them to come close to your home.
- Don�t allow your dogs and cats to wander freely or to capture and eat rodents.
- If you think that your pet may have eaten rodents, consult your veterinarian about possible preventive treatments.
- Wash your hands with soap and warm water after handling dogs or cats, and before handling food.
- Teach children the importance of washing hands to prevent infection.
-
Do not collect or eat wild fruits or vegetables picked directly from the ground.
All wild-picked foods should be washed carefully or cooked before eating.
Article: Echinococcus, Healthline.
INDEX
https://www.healthline.com/health/echinococcus
Medically reviewed by -- Judi Marcin, MD on June 2, 2016
Written by MaryAnn DePietro
Echinococcus is an infection caused by a parasitic tapeworm from the Echinococcus genus.
A few different types of tapeworms can cause echinococcus in humans, including:
E. granulosus,
E. multilocularis, and
E. vogeli.
In some cases, the organs affected depend on which type of tapeworm has caused your infection.
The infection is rare in the United States.
It occurs more often in the Mediterranean, Middle East, Africa, and Central Asia.
If left untreated, it can be fatal.
With treatment, your outlook may be good.
What are the symptoms of echinococcus?
Your symptoms will vary depending on which organs are affected.
According to Stanford University:
The infection affects the liver in about 75 percent of people who contract it.
Symptoms may include pain in your abdomen and the formation of cysts on your liver.
The infection affects the lungs in about 22 percent of people who contract it.
Respiratory symptoms may include chest pain and coughing up bloody mucus.
Other areas of your body can also be affected, including your skin, spleen, or kidneys.
What causes echinococcus?
If a parasitic tapeworm infects you, echinococcus will develop.
The parasite enters a host, which is usually an animal, such as a dog, sheep, or goat.
The worm lives in the bowels of the animal and releases its eggs into the animal�s feces.
You�re most likely to contract the infection when you eat food that has been contaminated with animal feces.
After eating contaminated food, the incubation period is usually a few months long.
This means it takes a few months before symptoms appear.
Certain strains of the parasite can have a longer incubation period that may last up to a few years.
How is echinococcus diagnosed?
Your doctor may ask you about your symptoms and perform medical tests to diagnose your infection.
For example, they may use a chest X-ray to rule out other types of infection.
Your doctor may also use an abdominal MRI or CT scan to make their diagnosis.
Because the incubation period can be long, echinococcus parasites may be discovered while your doctor is performing medical tests for other reasons.
How is echinococcus treated?
Medication is almost always used to treat echinococcus.
... your doctor may prescribe mebendazole or albendazole.
They may also recommend taking anti-inflammatory medication to treat inflammation of your organs caused by the parasite. Sometimes chemotherapy medications can be used to treat organ cysts caused by the parasite.
Surgery
In some instances, your doctor may recommend surgery to treat cysts caused by the infection.
If the infection has affected your brain and fluid has accumulated there, your doctor may also recommend surgery to install a shunt. This device is used to drain fluid from your brain.
How is echinococcus prevented?
... Removing the worms from dogs can help stop the spread of infection.
Correct disposal of animal feces can reduce exposure to tapeworm eggs.
Proper handling of cattle at farms and slaughterhouses is also essential.
This includes enforcing meat inspection procedures.
Avoiding undercooked or raw beef, pork, and fish can also help you avoid echinococcus.
Washing fruits and vegetables, especially in areas where the tapeworm is common, may help prevent infection.
Article: Parasites of the Liver � epidemiology, diagnosis
and clinical management in the European context.
INDEX
https://www.sciencedirect.com/science/article/pii/S016882782100115X
pdf LINK: https://www.sciencedirect.com/science/article/pii/...main.pdf
Lynn Peters, Sanne Burkert, Beate Gr�ner
University Hospital of Ulm,
Department of Internal Medicine III,
Division of Infectious Diseases,
Albert-Einstein-Allee 23, 89081 Ulm, Germany
(There are many detailed charts referencing parasites to symptoms.
There are 140 references, many with downloadable PDF versions.)
albendazole (ABZ)
benzimidazole (BMZ)
anthelmintic drugs (BMZ, possibly combined with praziquantel)
Abstract
Parasites in the liver cause significant global morbidity and mortality, as they can lead to recurrent cholangitis, cirrhosis, liver failure and cancer. Due to climate change and globalisation, the incidence is increasing, especially in Europe. Correct diagnosis is often delayed because clinicians are unfamiliar with respective entities. Therefore, this review aims at providing a clinical picture of hepatic parasites for clinicians, in order to bring these neglected parasitic liver diseases into the spotlight of hepatologic stakeholders in Europe.
1. Introduction
The liver is crucially involved in various parasitic infections.
For orally transmitted parasites, such as Echinococcus spp., liver flukes, Ascaris lumbricoides and Entamoeba histolytica, it is the first solid organ encountered after mucosal penetration, either directly or with the portal-venous blood flow. Other parasites reach the liver after the larvae penetrate the skin (schistosomiasis).
Recently, it has been argued that the liver offers a favourable immunological environment for parasites, as tolerance instead of immunity is the preferred immunological response to exogenous microorganisms. In addition, parasites have evolved complex mechanisms to alter the host�s immune response to overcome defence mechanisms. This allows for parasitic maturation (flukes) or proliferation (Echinococcus spp., amoebiasis) in the hepatic tissue.
Although hepatic parasites cause a significant global burden of disease, therapeutic options are limited, vaccines are not expected to be available soon due to the complex immunology and low economic incentive. Furthermore, the clinical presentation is often non-specific or asymptomatic, hampering diagnosis. In this review, we want to provide clinical guidance by presenting the most important parasitic infections of the liver, with the main epidemiological focus on Europe. Other parasitic infections such as visceral leishmaniasis, malaria, cryptosporidiosis or toxoplasmosis can also affect the liver, however, they usually cause a systemic inflammation and are hence not the main focus of this review. Table 1 summarises differential diagnoses of hepatic parasites from a clinical perspective, parasitological details are listed in table 2.
2. Hepatopathic Helminths
2.1. Cestodes of the liver: Echinococcus spp.
Human echinococcoses are zoonoses caused by the larval forms (metacestodes) of the cestode species (spp.) of the genus Echinococcus. Cystic echinococcosis (CE), caused by E. granulosus sensu lato, exceeds alveolar echinococcosis (AE), caused by E. multilocularis, in prevalence and geographic distribution. AE is restricted to the northern hemisphere within temperate climate zones. Central Asia has the highest prevalence of both diseases. In Europe, CE is endemic in Mediterranean and Eastern countries, while AE occurs in Western-Central, Baltic, and Eastern countries, as depicted in figure 1.
Echinococcoses have a substantial global public health impact.
Both AE and CE are considered orphan diseases, yet account for approximately 871,000 disability-adjusted life years (DALYs), which is still assumed to be largely underestimated. Despite their non-tropical distribution, echinococcoses are considered Neglected Tropical Diseases (NTDs). Due to scant data, diagnosis and treatment are guided by expert consensus led by recommendations of the WHO-IWGE (Informal Working Group on Echinococcosis), which are currently under revision. An �international consensus on terminology to be used in the field of echinococcosis� was recently published to harmonise globally used terms.
Echinococcus spp. depend on different mammals to complete their life cycles:
adult worms live in the small intestines of carnivores, their definite hosts, such as dogs or foxes. Matured eggs are released with their faeces and can be ingested by a suitable intermediate host (e.g. small rodents for E. multilocularis and ungulates for E. granulosus), where the eggs hatch and the larvae penetrate the intestinal wall. After migration with the host�s circulation and further maturation, Echinococcus spp. develop as lesions in different organs. The consumption of cyst-containing organs re-infects definite hosts and closes the parasitic life cycle. Humans act as so-called accidental intermediate hosts, acquiring the infection by ingestion of infective eggs and represent a dead-end host. Based on this life cycle, public health approaches for protecting the vulnerable population require basic hygiene regarding animal contact, sheep vaccination (CE), deworming domestic dogs (CE and AE) or fox-baiting with praziquantel (AE), as well as screening based on risk factors.
Although often discussed together, CE and AE are two distinct chronic diseases with different clinical features and treatment approaches: CE is generally considered benign with clearly delimited cystic lesions, yet causing a substantial medical and economic impact due to the cosmopolitan distribution. In contrast, AE develops as lesions formed by micro-cysts, appearing more solid and tumour-like, with the potential to infiltrate and metastasise, for which it is termed a malignant parasitosis. Therefore, diagnostic and clinical management should be carefully distinguished and left to specialist care. In this review, we discuss aspects of the (changing) epidemiology, clinical features, diagnostics and treatment of CE and AE in the European context.
2.1.1. Echinococcus granulosus sensu lato (cycstic Echinococcosis)
2.1.1.1. Epidemiology
Human CE is highly endemic in pastoral communities worldwide where close contact between humans, livestock and dogs is common. ...
2.1.1.2. Clinical features
Approximately 60�75% of CE cases are incidental findings, especially during the early stages of infection. Most CE-cases are diagnosed in adulthood. CE cysts can occur in all organs, but mostly affect the liver (70%), lungs (20-30%) or both. Depending on site and size of manifestations, symptoms result from compression or displacement of healthy tissue. Accordingly, patients may present with upper abdominal discomfort and biliary obstruction caused by cystobiliary fistula, leading to jaundice and/or cholangitis. Further complications include cyst rupture, inducing fever, urticaria, eosinophilia and anaphylaxis. ..
2.1.1.3. Diagnostics
The diagnosis of CE is primarily based on imaging techniques.
Serology can be useful to confirm the diagnosis of CE in unclear cases, but has a variable sensitivity: false-negative results are frequent in case of young, inactive or extra-hepatic cysts; a positive serology does not correlate with viability, as it can persist for years even after curative surgery and is hence inappropriate for follow-up.
Ultrasound (US) is the standard investigation for the diagnosis of hepatic CE.
Pathognomonic US (Ultrasound) features of CE cysts are listed in table 3.
The depicted classification based on cyst�s morphology, size, number and localisation allows to differentiate between active, transitional and inactive cysts and guides further management.
Other imaging techniques of hepatic CE lesions include magnetic resonance imaging (MRI) and computerised tomography (CT), which are mainly used for pre-operative evaluation or in case of complications; for diagnosis and follow-up of CE patients, they play a secondary role.
(TESTING)
Ultimately, if a case remains unclear, parasitological confirmation can be achieved by cytological examination of cyst material for brood capsules or protoscoleces, or by molecular analysis. Cyst puncture in suspected CE should only be done with both benzimidazole (BMZ)-pretreatment and precaution for possible anaphylactic reaction.
2.1.1.4. Treatment
Clinical decision-making for uncomplicated liver CE is based on US (Ultrasound) staging.
The goals of hepatic CE treatment are the complete elimination of viable parasitic cells, prevention of recurrence and consequently minimising mortality and morbidity. To achieve these aims, no "one-size-fits-all" approach exists, and the appropriate clinical management must be chosen considering disease-specific characteristics (cyst stage, number, size, site and presence of complications, cf. Table 3) and the patient�s clinical conditions, as well as local medical and surgical expertise.
There are currently four different management options available:
a) surgery,
b) percutaneous treatment,
c) medical treatment with anthelmintic drugs (BMZ, possibly combined with praziquantel), and
d) watch and wait for inactive cysts.
Surgery is the first therapeutic choice for large and complicated cysts,
i.e. cysts at risk of rupture or if fistulation or infection occurs. For CE2 and CE3b cysts, surgery should be evaluated.
For CE1 and CE3a cysts, percutaneous treatment is an option, aiming at the destruction of the germinal layer, either by performing puncture, aspiration, (injection and re-aspiration) (PA(IR)) or through the evacuation of the entire endocyst (modified catheterization technique). Excluding cysto-biliary fistulae before injecting any scolecidal agent is mandatory to prevent complications. Further findings restricting the feasibility of percutaneous aspiration are a subcapsular or extrahepatic localisation, as it increases the risk of leakage and dissemination into the adjacent cavity, CE2 and CE3a stage, and a previous history of hypersensitivity after cyst manipulation.
Small cysts may respond to medical therapy alone and thus do not justify the procedure-related risk. Medical treatment with BMZ, preferably albendazole (ABZ), is used to induce cyst inactivation, resulting in CE4 cyst resemblance, and is most effective in small CE1 and CE3a cysts, but often fails in the case of large cysts.
Recurrence is observed most commonly in conservatively treated CE2 and CE3b cysts.
BMZs are only parasitostatic, hence, regular sonographic follow-up is required to detect recurrence orreactivation promptly. If a solid stage is reached spontaneously, reactivation is rare. Despite the mentioned drawbacks, BMZ treatment remains the main treatment option in disseminated or inoperable CE.
In case of invasive procedures, prophylactic BMZ is required to avoid secondary echinococcosis potentially arising from spillage of viable larvae (brood capsules or protoscoleces). BMZ should be administered at least one day before and continued for at least 1-3 months after the procedure [11,35]. Praziquantel might enhance the effect of ABZ and is therefore recommended in some centres for peri-interventional prophylaxis [39].
2.1.2. Echinococcus multilocularis (Alveolar Echinococcosis)
2.1.2.1. Epidemiology and clinical impact
Human alveolar echinococcosis (AE) is the most lethal parasitic zoonosis in Europe.
If left untreated, the 10-year mortality rate can reach 90%. AE is considered an emerging disease, with an annual incidence of approximately 18,000 cases globally, of which 91% occur in China. In Europe, cases in the hitherto endemic area of Central Europe (France, Switzerland, Germany and Austria) are increasing in number. Moreover, the geographical distribution is expanding to countries previously considered AE-free like Poland, Slovakia, Hungary and the Baltic region, challenging respective health care systems.
Key risk factors for acquiring AE in Europe are being a farmer, owning a dog or cat or having a kitchen garden. Furthermore, the incidence of AE is higher among immunodeficient patients, who often show atypical presentations. A genetic susceptibility associated with an altered immune response was observed
2.1.2.2. Clinical presentation
Due to the slow growth of AE larvae, first symptoms can arise after several years of latency.
European patients are often older than 50 years and AE in children is rare.
Interestingly, in China, the average age at first diagnosis is significantly younger compared to Europe, and disease is often advanced, requiring a more invasive treatment approach.
Early symptoms are mostly non-specific including fatigue, abdominal pain or jaundice. One third of all cases is asymptomatic and diagnosed incidentally. Upon diagnosis, parasitic liver lesions are often extensive and infiltrate neighbouring structures, limiting treatment options. Common complications are
- portal vein thrombosis with consecutive portal hypertension,
- biliary duct obstruction with a risk for cholangitis and
- bacterial superinfection
in advanced lesions with considerable necrosis.
Since AE has the potential to metastasise, further symptoms depend on the organs involved.
2.1.2.3. Diagnosis
Diagnosis of AE is multimodal, based on clinical presentation along with epidemiological data, typical imaging signs, and serological tests. One finding on its own might be misleading, ... Serologic and histologic ormolecular confirmation is central. A two-step approach is recommended, using a high sensitivity screening test followed by a more specific confirmatory test, resulting in both high sensitivity and specificity of nearly 100% [63]. Still, there might be cross-reactivity with CE resulting in misinterpretation. Confirmation of AE can be achieved by histopathological examination including specific immunohistochemistry or nucleic acid detection in a clinical sample. An US (Ultrasound)-guided 0core-needle biopsy is an effective diagnostic tool to achieve a definitive diagnosis in hepatic AE. Based on the respective findings, AE can be classified as possible, probable or confirmed, defining the requirement of treatment
The morphology of AE lesions in different imaging modalities is shown in table 5.
US (UltraSound) is an important tool, yet findings are not pathognomonic, as opposed to CE.
Its main significance lies in the early detection of an often irregular lesion with a mixed echogenic pattern, calcification and an undefined margin, triggering further diagnostics. Other lesions show a resemblance with haemangiomas or metastases. Contrast-enhanced US (Ultrasound) (CEUS) may facilitate the confirmation of AE, since respective lesions do not show central contrast enhancement.
In contrast to CE, AE lacks a cystic appearance.
Therefore, sonographic diagnosis is often challenging for clinicians unfamiliar with the disease.
A CT, particularly for heavily calcified lesions, or MRI scan of the abdomen are the imaging techniques of choice. In analogy to the TNM-classification, a PNM-classification can be deduced from imaging to guide treatment (cf. Table 4). Staging is completed by a chest x-ray and a cerebral CT. Alternatively, a [18F]-fluorodeoxyglucose positron emission tomography (18F-FDG-PET) can be combined with a full-body CT-scan. FDG enrichment surrounding AE lesions is interpreted as larval metabolic activity and can serve as a follow-up tool. ...
2.1.2.4. Treatment
The key concept of AE treatment is a multidisciplinary approach and requires �personalised medicine�.
... The curative approach consists of radical surgery, completely removing all lesions including satellite lesions, followed by a 2-year course of BMZ. ... remarkable regression of AE liver lesions under strict BMZ treatment can be seen, allowing for complete surgical resection after months or even years (unpublished data). ...
However, upon diagnosis, the majority of patients is inoperable due to the involvement of liver vessels or bile ducts and therefore need long-term, mostly life-long BMZ-treatment. Under sufficient BMZ-treatment, FDG-uptakes should decrease or even vanish, corresponding to a suppressed periparasitic inflammatory activity. ....
2.1.2.5. Follow-Up and complications
All AE patients should be monitored by US (Ultrasound) at frequent intervals and by PET/CT and/or MRI every 2-3 years to evaluate disease recurrence or progression. Monitoring serology after surgery and/or BMZ-therapy is useful, as surgical removal of the lesion may result in seronegativity. After several years of BMZ treatment in stable AE without complications, a structured treatment interruption can be discussed.
Biliary complications, such as obstruction causing jaundice and cholangitis, are common in AE and occur in 10-30 % of patients. Especially late biliary complications (after more than 3 years of treatment) are associated with high mortality. Patients with acute complications might require hospitalisation for endoscopic interventions and antibiotic treatments. ...
2.2. Trematodes of the liver
Trematodes, or flukes, are flatworms which contain a snail in their life cycle.
They cause significant global morbidity and mortality, as they can lead to fibrosis, cirrhosis and cancer.
In recent years, especially foodborne trematodes have been on the rise, with an increase both in incidence and geographical distribution (cf. Figure 2). Currently, trematodes are leading to 200,000 illnesses annually and over 7,000 deaths ...
2.2.1. Fasciola hepatica and Fasciola gigantica
Fascioliasis can be caused by the flatworms Fasciola hepatica and Fasciola gigantica.
It is a widely spread zoonosis and ruminants serve as natural definite hosts. Human fascioliasis mainly occurs in rural areas where sheep and cattle husbandry is common. The animals� excreta contain eggs that, if released into freshwater, hatch and infect water snails, the intermediate host. After maturation and multiplication, larvae are released into the water and develop into metacercariae, which encyst attaching to aquatic plants. With the ingestion of respective plants, the larvae reach the small intestine, penetrate the wall and migrate through the peritoneum and heaptic tissue to the bile ducts, where they mature and produce eggs, closing the infectious cycle. Human infections are caused by undercooked water plants (e.g. watercress), plants that need frequent irrigation and are manured with animal excreta and, to a lesser extent, by contaminated drinking water. ...
2.2.2. Clonorchis sinensis, Opisthorchis viverrini and Opisthorchis felineus
The so-called small liver flukes of the families Clonorchis and Opisthorchis are mainly spread in Asia.
Eggs are excreted into freshwater with the faeces of dogs, cat, birds, reptiles or other definitive hosts. Larvae hatch and infect water snails, the first intermediate host, where they multiply. They ultimately leave the snail and penetrate the skin of their second intermediate host, mainly fish, where they encyst within the muscular tissue. After consumption, the larvae are released within the definitive host�s digestive tract and migrate to the liver using the bile duct. Humans act as accidental definitive hosts and infections occur after consumption of poorly cooked fish. Thus, populations that depend on fishing as a livelihood are particularly affected. Salting, drying, marinating or short-time freezing does not affect the viability of the larvae. ...
2.2.3. Schistosoma mansoni and S. japonicum
According to the WHO, approximately 240 million people are infected with schistosomes globally.
As a water-based NTD, endemic areas are found in tropic and subtopic climate zones on every continent, mainly in Sub-Saharan Africa and South America. The infectious cycle requires freshwater contact: different water snails, the intermediate hosts, release cercariae into the water which penetrate human skin, migrate through the lungs as immature schistosomulae and mature in the liver, to finally settle in abdominal vessels. ...
Apart from a possible dermatitis resulting from larval penetration, first symptoms usually occur 4-6 weeks after infection with the first shedding of eggs. This causes a strong immune reaction resulting in a flu-like syndrome called Katayama-fever, ....
2.3. Nematodes of the liver: Ascaris lumbricoides
Currently, 800 million people worldwide are infected with Ascaris lumbricoides.
The geographical distribution of ascariasis is linked to low socio-economic standards with insufficient hygiene practices due to poor housing and sanitation, promoting the parasite cycle. ...
3. Protozoan parasites: Entamoeba histolytica
Amoebiasis is caused by the protozoa Entamoeba histolytica and occurs in humans and primates.
The burden of disease is considerably high with an estimated annual 50 million infections and 55,000 deaths. Globally, impoverished communities with insufficient sanitary facilities are most affected, since E. histolytica is mainly transmitted faecal-orally.
KEY POINTS
...
AE has a high mortality if left untreated, hence early diagnosis is crucial, requiring at least imaging and serological testing. Staging is mandatory to guide treatment, using CT, MRI or preferably PET-CT scan. For early stages, complete resection followed by a 2-year course of albendazole is recommended. Late stages require long-term, often life-long medical treatment with albendazole. Challenges are the management of biliary and vascular complications and the lack of alternative medical options in case of albendazole intolerance. ...
Article: Echinococcosis, WHO World Health Organization.
INDEX
https://www.who.int/news-room/fact-sheets/detail/echinococcosis
by World Health Organization
23 March 2020
Key facts
-
Human echinococcosis is a parasitic disease caused by tapeworms of the genus Echinococcus.
-
The two most important forms in humans are cystic echinococcosis (hydatidosis / CE) and alveolar echinococcosis (AE).
-
Humans are infected through ingestion of parasite eggs in contaminated food, water or soil, or after direct contact with animal hosts.
-
Echinococcosis is often expensive and complicated to treat and may require extensive surgery and/or prolonged drug therapy.
-
Prevention programmes focus on deworming of dogs, which are the definitive hosts.
In the case of cystic echinococcosis preventive measures also include, deworming dogs, slaughterhouse hygiene, and public education.
-
More than 1 million people are affected with echinococcosis at any one time.
Human echinococcosis is a zoonotic disease (a disease that is transmitted to humans from animals) that is caused by parasites, namely tapeworms of the genus Echinococcus. Echinococcosis occurs in 4 forms:
-
cystic echinococcosis, also known as hydatid disease or hydatidosis, caused by infection with a species complex centred on Echinococcus granulosus;
-
alveolar echinococcosis, caused by infection with E. multilocularis;
- two forms of neotropical echinococcosis: polycystic caused by infection with E. vogeli; and
-
- unicystic caused by E. oligarthrus.
The two most important forms, which are of medical and public health relevance in humans, are cystic echinococcosis (CE) and alveolar echinococcosis (AE).
Transmission
A number of herbivorous and omnivorous animals act as intermediate hosts of Echinococcus.
They become infected by ingesting the parasite eggs in contaminated food and water, and the parasite then develops into larval stages in the viscera.
>Carnivores act as definitive hosts for the parasite, and harbour the mature tapeworm in their intestine.
The definitive hosts are infected through the consumption of viscera of intermediate hosts that contain the parasite larvae.
Humans act as so-called accidental intermediate hosts in the sense that they acquire infection in the same way as other intermediate hosts, but are not involved in transmitting the infection to the definitive host.
Several distinct genotypes of E. granulosus are recognised, some having distinct intermediate host preferences. Some genotypes are considered species distinct from E. granulosus. Not all genotypes cause infections in humans. The genotype causing the great majority of cystic echinococcosis infections in humans is principally maintained in a dog�sheep�dog cycle, yet several other domestic animals may also be involved, including goats, swine, cattle, camels and yaks.
Alveolar echinococcosis (AE) usually occurs in a wildlife cycle between foxes or other carnivores with small mammals (mostly rodents) acting as intermediate hosts. Domesticated dogs and cats can also act as definitive hosts.
Signs and symptoms
Cystic echinococcosis / hydatid disease
Human infection with E. granulosus leads to the development of one or more hydatid cysts located most often in the liver and lungs, and less frequently in the bones, kidneys, spleen, muscles and central nervous system.
The asymptomatic incubation period of the disease can last many years until hydatid cysts grow to an extent that triggers clinical signs, however approximately half of all patients that receive medical treatment for infection do so within a few years of their initial infection with the parasite.
Abdominal pain, nausea and vomiting are commonly seen when hydatids occur in the liver.
If the lung is affected, clinical signs include chronic cough, chest pain and shortness of breath.
Other signs depend on the location of the hydatid cysts and the pressure exerted on the surrounding tissues.
Non-specific signs include anorexia, weight loss and weakness.
Alveolar echinococcosis (AE)
Alveolar echinococcosis is characterized by an asymptomatic incubation period of 5�15 years and the slow development of a primary tumour-like lesion which is usually located in the liver. Clinical signs include weight loss, abdominal pain, general malaise and signs of hepatic failure.
Larval metastases may spread either to organs adjacent to the liver (for example, the spleen) or distant locations (such as the lungs, or the brain) following dissemination of the parasite via the blood and lymphatic system. If left untreated, alveolar echinococcosis is progressive and fatal.
Distribution
Cystic echinococcosis is globally distributed and found in every continent except Antarctica.
Alveolar echinococcosis is confined to the northern hemisphere, in particular to regions of China, the Russian Federation and countries in continental Europe and North America.
In endemic regions, human incidence rates for cystic echinococcosis can reach more than 50 per 100 000 person-years, and prevalence levels as high as 5%�10% may occur in parts of Argentina, Peru, East Africa, Central Asia and China. In livestock, the prevalence of cystic echinococcosis found in slaughterhouses in hyperendemic areas of South America varies from 20%�95% of slaughtered animals.
The highest prevalence is found in rural areas where older animals are slaughtered.
Depending on the infected species involved, livestock production losses attributable to cystic echinococcosis result from liver condemnation and may also involve reduction in carcass weight, decrease in hide value, decrease of milk production, and reduced fertility.
Diagnosis
Ultrasonography imaging is the technique of choice for the diagnosis of both cystic echinococcosis and alveolar echinococcosis in humans. This technique is usually complemented or validated by computed tomography (CT) and/or magnetic resonance imaging (MRI) scans.
Cysts can be incidentally discovered by radiography.
Specific antibodies are detected by different serological tests and can support the diagnosis.
Early detection of E. granulosus and E. multilocularis infections, especially in low-resource settings, is still needed to aid in the selection of clinical treatment options.
Treatment
Both cystic echinococcosis and alveolar echinococcosis are often expensive and complicated to treat, sometimes requiring extensive surgery and/or prolonged drug therapy. There are 4 options for the treatment of cystic echinococcosis:
-
percutaneous treatment of the hydatid cysts with the PAIR
--- (Puncture, Aspiration, Injection, Re-aspiration) technique;
- surgery
- anti-infective drug treatment
- �watch and wait�.
The choice must primarily be based on the ultrasound images of the cyst, following a stage-specific approach, and also on the medical infrastructure and human resources available.
For alveolar echinococcosis, early diagnosis and radical (tumour-like) surgery followed by anti-infective prophylaxis with albendazole remain the key elements. If the lesion is confined, radical surgery can be curative.
Unfortunately in many patients the disease is diagnosed at an advanced stage.
As a result, if palliative surgery is carried out without complete and effective anti-infective treatment, frequent relapses will occur.
Health and economic burden
Both cystic echinococcosis and alveolar echinococcosis represent a substantial disease burden.
Worldwide, there may be in excess of 1 million people living with these diseases at any one time.
Many of these people will be experiencing severe clinical syndromes which are life-threatening if left untreated. Even with treatment, people often face reduced quality of life.
For cystic echinococcosis, there is an average of 2.2% post-operative death rate for surgical patients and about 6.5% of cases relapse after an intervention, thereby requiring prolonged recovery time.
The 2015 WHO Foodborne Disease Burden Epidemiology Reference Group (FERG) estimated echinococcosis to be the cause of 19,300 deaths and around 871,000 disability-adjusted life-years (DALYs) globally each year.
Annual costs associated with cystic echinococcosis are estimated to be US$ 3 billion for treating cases and losses to the livestock industry.
Surveillance, prevention and control
Robust surveillance data is fundamental in order to show burden of disease and to evaluate progress and success of control programmes. However, as for other neglected diseases which are focused in underserved populations and remote areas, data is especially scarce and will need more attention if control programmes are to be implemented and measured.
Cystic echinococcosis / hydatid disease (CE)
Surveillance for cystic echinococcosis in animals is difficult because the infection is asymptomatic in livestock and dogs. Surveillance is also not recognized or prioritized by communities or local veterinary services.
Cystic echinococcosis is a preventable disease as it involves domestic animal species as definitive and intermediate hosts. Periodic deworming of dogs with praziquantel (at least 4 times per year), improved hygiene in the slaughtering of livestock (including the proper destruction of infected offal), and public education campaigns have been found to lower and, in high-income countries, prevent transmission and alleviate the burden of human disease.
Vaccination of sheep with an E. granulosus recombinant antigen (EG95) offers encouraging prospects for prevention and control. The vaccine is currently being produced commercially and is registered in China and Argentina. Trials in Argentina demonstrated the added value of vaccinating sheep, and in China the vaccine is being used extensively.
A programme combining vaccination of lambs, deworming of dogs and culling of older sheep could lead to elimination of cystic echinococcosis disease in humans in less than 10 years.
Alveolar echinococcosis (AE)
Prevention and control of alveolar echinococcosis is more complex as the cycle involves wild animal species as both definitive and intermediate hosts. Regular deworming of domestic carnivores that have access to wild rodents should help to reduce the risk of infection in humans.
Deworming of wild and stray definitive hosts with anthelminthic baits resulted in significant reductions in alveolar echinococcosis prevalence in European and Japanese studies. Culling of foxes and unowned free-roaming dogs appears to be highly inefficient. The sustainability and cost�benefit effectiveness of such campaigns are controversial.
WHO and country response
Strengthening echinococcosis prevention and control
Informal Working Groups on Echinococcosis were founded in 1985 under the auspices of the WHO.
For 10 years, under the leadership of Professor J. Eckert (University of Zurich, Switzerland), the groups organised meetings of specialists and promoted international scientific exchange and co-operation in the field of echinococcosis research. In 1995, the WHO modified the structure of the groups and transformed them into a single group, the WHO Informal Working Group on Echinococcosis (WHO-IWGE). The mission of the WHO-IWGE is to strengthen prevention and control of echinococcosis through effective collaboration with strategic partners and relevant sectors. The current Chair of the WHO-IWGE is Professor Thomas Junghanss (Heidelberg University, Germany), and Co-Chair is Professor Okan Akhan (Hacettepe University, Turkey).
The WHO-IWGE developed in 1995 a standardized classification of cystic echinococcosis (CE) that could be applied in all settings. In 2009, the consensus for diagnosis and treatment of CE and alveolar echinococcosis (AE) reached by the WHO-IWGE was published (Brunetti et al., 2010), providing updated guidelines for diagnosis and treatment.
The WHO-IWGE is in the process of reviewing the diagnosis and associated clinical management of echinococcosis and elaborating technical manuals with practical applicability. Several workings groups have been created to cover the different aspects of the diseases and are working on creating those documents. The group is also working to promote the collection and mapping of epidemiological data.
Building capacity to enhance early diagnosis and clinical management of CE
WHO has been asked by the endemic countries to provide support on early diagnosis and clinical management of cystic echinococcosis. WHO supports capacity building through training courses targeting medical and paramedical personnel, focused on the clinical management of cystic echinococcosis in rural areas of affected countries. This is an integral component to support universal health coverage.
Morocco undertook a project aimed at decentralizing diagnostic and therapeutic techniques and promoting the PAIR (puncture, aspiration, injection, re-aspiration) strategy in rural and hyperendemic areas.
Mongolia has recognized the importance of echinococcosis as a public-health problem and, at the request of the Ministry of Health, WHO in 2013 conducted an initial situation analysis. The analysis focused on implementing early diagnosis and building a basic surveillance system covering humans and animals to understand the actual burden of the disease.
A cross-sectional study conducted in Bulgaria, Romania and Turkey in 2014-2015, found that the true burden of CE is poorly understood and that many cases remain asymptomatic, with no appropriate medical diagnosis and treatment. The study assessed the prevalence of the disease among rural populations in the three countries.
In the Americas, a cystic echinococcosis control manual was produced by the Pan American Health Organization / WHO Regional Office for the Americas (OPS) and Panaftosa in 2017. It has been published in Spanish.
Working with veterinary and food safety authorities to support the development of echinococcosis control programmes
The transmission cycle of cystic echinococcosis (CE) involves dogs, and intermediate hosts, commonly sheep. In order to break the transmission cycle, control measures need to consider those animals. Control measures in dogs and sheep, as part of a One-Health approach include the deworming of dogs with praziquantel at least 4 times per year and the vaccination of lambs with EG95 vaccine.
Under the umbrella of One Health, WHO and its partner, the World Organization for Animal Health (OIE) are supporting the development of echinococcosis control programs including animal interventions. Joint meetings are being held regularly and technical support is provided to promote control, for example in the Central Asia and South Caucasus countries.
WHO assists countries to develop and implement pilot projects leading to the validation of effective cystic echinococcosis control strategies. Working with the veterinary and food safety authorities as well as with other sectors is essential to attain the long-term outcomes of reducing the burden of disease and safeguarding the food value chain.
WHO is supporting individual countries to develop their CE control program such as in Mongolia. In 2018, a multidisciplinary stakeholder meeting was convened in Ulaanbaatar to start developing the National Action Plan for control of echinococcosis. No significant investment for echinococcosis has been made, and therefore programmatic steps have been progressing slowly but WHO continues to bring the stakeholders together and further actions have been agreed in 2019. WHO has also facilitated the validation of diagnostic tests used for echinococcosis in dogs that is important for surveillance, and create a baseline in Bayankhongor province of Mongolia.
China is integrating echinococcosis prevention, control and treatment in their economic and development plans to raise attention to the vast problem in the country, especially the Tibetan plateau, as well as in the Central Asian Republics.
WHO is promoting One-Health approaches, such as the one developed by Dr Larrieu in the Argentinian Patagonia which involves community health workers, dog deworming and sheep vaccination.
Improving data on CE
Surveillance data is key to understand the disease epidemiological situation and taking action in the risk areas, and for setting up priorities. Data is also necessary to monitor the progress of interventions and evaluate the outcomes of control actions.
Indicators are specific variables that assist with the data analysis and provide tools for health authorities and people involved in disease control. WHO has defined a new set of indicators at country and global level for CE and is developing reporting systems to guide and assist the countries on data collection and reporting.
At global level, the indicators are
1- Number of endemic countries for CE, and
2- Number of countries with intensified control in hyper endemic areas.
A hyperendemic area has been defined as an area with an annual incidence of 5 human cases/100,000 people.
At country level there are epidemiological indicators and control progress indicators.
The epidemiological indicators include a combination of passive and active surveillance.
The control indicators include impact and outcome indicators.
(1) One DALY (disability-adjusted life year) can be thought of as one lost year of �healthy� life.
The sum of these DALYs across the population, or the burden of disease, can be thought of as a measurement of the gap between current health status and an ideal health situation where the entire population lives to an advanced age free of disease and disability.
Article: A multiplex PCR for .. detection of .. Echinococcus multilocularis ..
INDEX
A multiplex PCR for differential detection of Echinococcus granulosus
sensu stricto, Echinococcus multilocularis and Echinococcus canadensis in China
Jing-Ye Shang, Guang-Jia Zhang, Sha Liao, Yan Huang, Wen-Jie Yu,
Wei He, Guang-You Yang, Tiao-Ying Li, Xing-Wang Chen, Bo Zhong,
Qian Wang, Qi Wang, Rui-Rui Li & Hao Wang
Infectious Diseases of Poverty volume 8, Article number: 68 (2019)
The developed multiplex PCR shows advantages in fast diagnosis and large-scale epidemiological investigation, which proven to be a promising tool utilized in clinic and surveillance system.
Echinococcosis, caused by the infection of one or more of nine species within the genus Echinococcus, is among the most neglected zoonoses distributed globally, bringing about great public health concerns and economic losses. In China, where 368 endemic counties distributed in 9 provinces with an estimated 166,098 cases nationally, four species coexisted. E. granulosus sensu strict (G1�3) and E. canadensis (G6�8, 10) infections lead to cystic echinococcosis (CE), which is the most major type of the disease. E. multilocularis infection result in alveolar echinococcosis (AE), also called as �parasite cancer�, is one of the most lethal parasitic infections in humans. ... Because the treatment principles and chemotherapeutic effects vary much between CE and AE, and the life cycles, transmission patterns and related risk factors of these species are quite different, the accurate detection and identification of the species are extraordinarily vital in effective treatment and targeted control of ecinococcosis. ...
The developed multiplex PCR method was used to test samples obtained from patients and different infected animals. ... DNA isolated from parasite lesions taken from humans and domestic animals was all successfully amplified, and the multiplex PCR identification results agreed with the initial sequencing results. ... Furthermore, of all the tested stool samples, 16 were found to contain adult worms of Echinococcus by visual and microscopic examination. Among the 16 positive samples, 13 were detected as E. multilocularis by the multiplex PCR, and the remained three presented negative both in the current assay and previous molecular identification. ...
The advantage of the multiplex PCR method becomes more obvious when it is used for the test of the causative pathogens in definitive hosts other than intermediate hosts, because miss detection of mixed species infections are more likely to happen in stools compared to tissues, even though this kind of samples count just for a small portion of the total. None of the fecal materials showed co-infection in the study owing to the lack of such samples, but the results of the spiked DNA samples have fully proved that the developed assay is capable of detecting double and triple mixed infections of the targeted species effectively. ...
The evaluation results based on various samples obtained from human and different animal hosts indicated that the multiplex PCR developed in this study is applicable for clinical and epidemiological use, particularly for the confirmation and classification of human echinococcosis. Further optimization will be implemented.
Conclusions
The new single-tube multiplex PCR method that allows rapid, accurate and simultaneous detection of E. granulosus s. s., E. multilocularis and E. canadensis was developed and assessed in the study. The results suggested that the method has potential application in fast detection and large-scale screening, which makes it a promising candidate as the key technology for clinical diagnosis and environmental monitoring.
Correspondence to
Yan Huang
https://idpjournal.biomedcentral.com/articles/
10.1186/s40249-019-0580-2/email/correspondent/c1/new
(Online e-mail form)
or
Bo Zhong
https://idpjournal.biomedcentral.com/articles/
10.1186/s40249-019-0580-2/email/correspondent/c2/new
(Online e-mail form)
Article: IDEXX Reference Laboratories introduces
new Echinococcus RealPCR Panel (2019).
INDEX
ONLY Veterinary applications.
https://ca.idexx.com/files/echinococcus-realpcr-panel-dx-update-ca-en.pdf
Ordering Information
Test code: EMPPE
Test name and components: Echinococcus RealPCR� Panel
Echinococcus multilocularis and Echinococcus spp. RealPCR� tests
Specimen requirements
The ideal specimen depends on the clinical manifestation:
�Patient with suspected alveolar or cystic echinococcosis:
aspirate of suspect cystic lesion on a sterile swab, in a sterile tube (RTT or WTT)
�Exposed animal without clinical signs (to evaluate for intestinal Echinococcus infection):
5 g (1 g minimum) fresh feces in a sterile container
Turnaround time: 1-3 working days
Ordering your tests online
Did you know that you can search for diagnostic tests, create requisitions, and review status and results
on vetconnectplus.ca?
Customer support services:
IDEXX supports your practice with our customer support, technical support, and medical consulting services team, including our diagnostic support veterinarians and board-certified veterinary specialists.
1-800-667-3411 -- Customer Support, Catherine McKiver.
Echinococcus multilocularis has recently been identified as an emerging disease of concern in Canada and the northern United States. This tapeworm, carried by wild canids, poses a significant zoonotic threat if appropriate preventive steps are not taken.
A recent prevalence study showed that an alarming 23% of wild canid feces in Ontario were positive for Echinococcus multilocularis. An earlier study of coyote carcasses from the Calgary and Edmonton, Alberta region showed a similar prevalence of 25.3%. To address concerns about the spread of Echinococcus in North America, IDEXX Reference Laboratories has responded quickly to develop and validate a test for Echinococcus. ..
Humans may become accidental hosts when they ingest the tapeworm eggs from infected feces.
This may occur when handling contaminated soil (e.g. gardening), eating unwashed vegetables grown in infected soil, or from fecal-oral transmission following handling of infected feces.
Alveolar echinococcosis (also known as hydatid disease) is a serious, and often fatal, complication of Echinococcus infection. Due to the slow growth of these multilocular hydatid cysts, clinical signs may not occur until 5-15 years after initial infection.
Other zoonotic Echinococcus species of importance in North America include Echinococcus granulosus and Echinococcus canadensis. The eggs and adult tapeworms of these species are morphologically identical and very closely related genetically. They are distinguished by differences in their intermediate hosts, geographic distribution and by which organs most commonly develop hydatid cysts.
E. canadensis is found mainly in northern North America.
The most common definitive hosts are coyotes and wolves, and the intermediate hosts are primarily moose and elk.
E. granulosus is primarily found in South and Central America, Africa, the Middle East, China, Italy, Spain, Greece, Russia and the southwestern United States (especially Arizona, New Mexico and California). Dogs, wild canids and cats serve as definitive hosts, while sheep, goats, swine and cattle serve as intermediate hosts. Due to the differences in intermediate hosts, pet dogs may be more likely to be infected with and transmit E. granulosus than E. canadensis.
Clinical signs in alveolar echinococcosis vary depending on the organ in which the cysts develop. The most common site is the liver. Clinical signs (vomiting, lethargy, inappetence, abdominal pain, and jaundice) and ultrasound findings (cystic masses) are similar to those seen with liver cancer. ... Clinical signs may not be seen until the cysts have grown large enough to cause a mass-effect, which may take years from initial infection.
In response to the concern regarding this emerging disease, IDEXX Reference Laboratories developed and validated an EchinococcusRealPCR� Panel in collaboration with researchers at the University of Guelph.
The panel includes both a species-specific real-time PCR test for E. multilocularis and a genus-level Echinococcus spp.test. The Echinococcus spp. test detects not only E. multilocularisbut also other clinically relevant Echinococcus species, such as E. canadensis and E. granulosus.
In dogs presenting with cystic masses suggestive of echinococcosis, the Echinococcus RealPCR� Panel can be performed on a specimen collected by fine-needle aspiration of the suspect mass, eliminating the need for a biopsy.
Additionally, the Echinococcus RealPCR Panel performed on a fecal specimen may detect chronic nonclinical shedders of Echinococcus spp. or may be used to distinguish Echinococcus spp. eggs from Taenia eggs when tapeworm eggs are identified on fecal flotation.
Eggs are stable for up to a year in cooler 15�C (60�F) moist environments and are able to withstand freezing temperatures.
Surgical excision, especially early in the course of the disease or when a solitary cyst is present, may be curative when combined with albendazole. When multiple cysts (as in alveolar echinococcosis) are present, surgery may not be possible and praziquantel may be a temporary palliative measure only.
Percutaneous draining of cysts by ultrasound guidance has also been found to be useful in treatment of echinococcosis in humans. Dogs with alveolar or cystic echinococcosis may also have a patent intestinal infection. Therefore, these dogs should also be treated with praziquantel to prevent zoonotic infections.
Article: Toxocariasis, Hydatid Disease of the Lung, ... and Pulmonary ..
INDEX
Toxocariasis, Hydatid Disease of the Lung, Strongyloidiasis, and Pulmonary Paragonimiasis
https://www.sciencedirect.com/topics/
medicine-and-dentistry/echinococcus-multilocularis
by Ayesha Mirza MD, Mobeen H. Rathore MD, CPE, FAAP, FIDSA, FACPE,
in Kendig & Chernick's Disorders of the Respiratory Tract in Children (Eighth Edition),
2012
Alveolar Hydatid Disease
Echinococcus multilocularis is a cestode that differs morphologically and biologically in its larval and adult stages from E. granulosus. The usual definitive host is the fox, with dogs and cats acting as sources of human infection in endemic areas. Intermediate hosts are rodents and humans. The larval stage develops normally in rodents, but humans are unusual and poor intermediate hosts. The disease is usually found across much of the Soviet Union, central Europe, northern Japan, Alaska, and northern Canada. Human disease is rare in the Western Hemisphere, but the cestode is endemic in the north-central United States and Canada.
The infection usually occurs during childhood.
... risk factors:
having a lifetime pattern of dog ownership,
tethering dogs near the house, and
living in a house built directly on the tundra rather than on gravel or permanent foundations,
---- thus allowing contact with contaminated dog feces.
Other implicated factors are
the drinking of unboiled melted snow and
the skinning of foxes.
The disease manifests usually between the ages of 19 and 40 years but has been seen in those as young as 5 years. The mean age at diagnosis in Alaska is 53 years.
The disease favors neither sex.
The larval cestode persists in its proliferative phase because of the inability of humans to provide the conditions necessary for normal development. Instead of developing a thick, laminated layer and growing into large, single cysts, the parasite has a thin, deficient ectocyst that grows and infiltrates into the surrounding tissues.
The growing cyst may have several small, fluid-filled pockets containing protoscoleces.
Because of its structure, this larval form is called an alveolar or multilocular hydatid.
It provokes a severe host reaction and becomes surrounded by an inflammatory or granulomatous reaction, instead of the fibrous host response seen with E. granulosus. A central area of necrosis is always seen.
The cyst is slow growing, behaves like a malignancy, and has been mistaken for carcinoma, which it can mimic clinically and microscopically. Untreated it can be just as devastating, with mortality rates as high as 80%.
The primary site of infection is the liver, where a dense honeycomb of small, multilocular cysts is formed.
The cyst appears as a solid cancerlike growth that may cavitate and attain massive size.
Through the inferior vena cava it may metastasize to distant organs.
Alveolar hydatid disease of the lung is invariably a metastatic focus.
Diagnosis is based on history of exposure, elevated serologic titers, and characteristic changes on radiographic studies. Physical signs are confusing, and subjective symptoms may be mild, vague, and ill defined. Patients present usually with asymptomatic hepatomegaly.
When symptoms are present, they are commonly related to the abdomen:
- mild epigastric and right upper-quadrant abdominal pain or distress,
- intermittent fever, and
- jaundice.
On radiologic examination, hepatomegaly and hepatic calcification are the most common findings. Typically, the diagnosis is made with abdominal radiographs that show scattered radiolucent areas surrounded with calcification, sometimes referred to as the �Swiss cheese� liver calcification pattern. This finding is pathognomonic, but at least 5 years of illness must elapse before calcification can be demonstrated. Without the characteristic radiographic study, the diagnosis is rarely made preoperatively. ...
Treatment is by surgery.
Early diagnosis is very important to permit resection before infiltration becomes too extensive. However, many cases are undiagnosed until they are well advanced and the hepatic lesions are unresectable.
At surgery, liver invasion is often more extensive than suggested by the degree of calcification on the radiograph. Complete excision is the only hope. Cure is possible when partial hepatectomy or hepatic lobectomy can remove all multilocular cysts and still preserve enough organ function. Still, radical hepatic resection is curative in only 20% of cases. Palliative measures are designed to ensure adequate bile drainage.
If surgery is unsuccessful or impractical, mebendazole is recommended at 40 mg/kg/day in divided doses for life, which may prevent progression of the primary lesion and metastasis and prolong life. Benzimidazole compounds are parasitostatic rather than parasitocidal for E. multilocularis. Thus, treatment with these agents implies lifelong application.
The overall success rate of such treatment ranges between 55% and 97%.
Hepatic toxicity with the use of this drug can develop without warning, however, and does not seem to be dose related or likely due to hypersensitivity. Hepatic function should be monitored the entire time the drug is administered.
Monitoring should be done weekly during the first month and monthly thereafter.
Amphotericin B has shown to have some benefit as salvage treatment.
Though not fulminating, the disease is ultimately fatal unless early surgical intervention can remove the parasite cyst. Patients have survived at least 16 years after diagnosis.
Death is due to
- liver failure;
- invasion of contiguous areas; and
- metastases to the lung, brain, and distant organs.
Article: Parasites in Food: Occurrence and Detection.
INDEX
https://www.sciencedirect.com/topics/
medicine-and-dentistry/echinococcus-multilocularis
by L.J. Robertson,
in Encyclopedia of Food and Health,
2016
Echinococcus multilocularis
The fox tapeworm, Echinococcus multilocularis, has a similar life cycle to that for E. granulosus but is mostly associated with a sylvatic life cycle, with foxes usually serving as definitive hosts. Other canids (e.g., dogs, raccoon dogs, wolves, and coyotes) may also act as definitive hosts. Various different genera of rodents (also some lagomorphs) may act as intermediate hosts, being infected by ingestion of eggs released from the tapeworms in the definitive hosts. A number of nonrodent mammals, including humans and pigs, may also be infected as aberrant or accidental intermediate hosts; in humans, this may result in the disease state known as alveolar echinococcosis (AE).
Data on the prevalence of AE in humans are scattered and patchy, probably partly due to diagnostic challenges, particularly in early stages of infection. E. multilocularis infection apparently does not occur in Australasia, Africa, and South or Central America, but countries in Asia and Europe, as well as North America, are important endemic areas.
While the tiny (3�6 mm) adult E. multilocularis tapeworms normally cause little harm to canine definitive hosts, in intermediate hosts, including humans, ingested eggs develop to oncospheres, which penetrate the intestinal wall and are carried via blood to, in particular, not only the liver but also other organs where they form multilocular cysts. From ingestion of eggs to onset of clinical symptoms in people may be from months to years, or even decades, depending on cyst location and speed of growth.
In most AE cases, metacestodes of E. multilocularis initially develop in the liver.
These cysts, varying from a few millimeters to 15�20 cm or more in diameter, can also reproduce aggressively by asexual lateral budding. This gradual invasion of adjacent tissue in a tumorlike manner is the basis for the severity of AE. Metacestodes may also spread from the liver to other organs, such as the lungs, spleen, heart, and kidney. Symptoms of severe hepatic dysfunction appear in the advanced clinical stage, in addition to symptoms from other affected organs. While there is negligible acute morbidity, the chronic morbidity of AE is severe and potentially fatal.
As with CE, the proportion of AE cases that are actually foodborne is difficult to estimate, as diagnosis usually occurs long after infection; it is difficult to associate an infection with a foodborne event many years previously. However, the tapeworm eggs may contaminate various types of food, including fruits and vegetables.
Although sensitive to desiccation and heat, the eggs are extremely tolerant of environmental conditions, including cold; freezing at - 20 �C does not affect egg infectivity. Thus, there is a large potential for foodborne infection via raw produce. However, there are currently no tools for detecting E. multilocularis eggs on food. ...
Article: Solitary Lucent Defect, Parasitic Cysts. (2019)
INDEX
https://www.sciencedirect.com/topics/
medicine-and-dentistry/echinococcus-multilocularis
by James C. Reed MD,
in Chest Radiology (Seventh Edition),
2019
Hydatid cysts are the result of infection with Echinococcus granulosus or Echinococcus multilocularis. Dogs or other carnivores are the primary host of these parasites, and sheep may be intermediate hosts. Humans are infected by the ingestion of contaminated food, and the parasite embryo passes through the duodenal mucosa into the portal vein to the liver.
The wall of a hydatid cyst has three layers.
The inner layer is a very thin, unicellular layer from which arise the scolices; the middle layer is a laminated, chitinous layer, which is the parasite (endocyst); and the third layer is a fibrous reaction of the host to the parasite. When they are intact, cysts may be filled with fluid and appear as a nodule or mass on the chest radiograph and a low attenuation cyst on CT.
After a cyst develops a communication with a bronchus, the radiologic appearance changes.
Introduction of air into the cyst causes separation of the fibrous and laminated layers of the cyst.
A small amount of air between the two layers leads to a lucent crescent, or the air meniscus sign.
This appearance might be mimicked by the development of a fungus ball in a preexisting cavity, but examination of previous studies should resolve this differential because the previous existence of a homogeneous circumscribed opacity would be evidence against the diagnosis of a fungus ball.
When the endocyst ruptures, the fluid drains into the tracheobronchial tree, leading to the radiologic appearance of an air-fluid level in a sharply defined lucent space. After the fluid has partially drained, the laminated, chitinous middle layer of the cyst separates from the fibrous layer. This permits the endocyst layer to separate from the outer wall and float on the remaining fluid.
It has a very characteristic chest radiographic and CT appearance that permits a specific diagnosis. This radiologic presentation has been described as the �water lily� sign and is distinctive for hydatid disease. It is very common for the scolices to disseminate through the bronchi with the development of multiple cysts.435 A history of having lived in an area of the world where hydatid disease is endemic is essential if the diagnosis is to be suspected.
The incidence of the disease is particularly high in Russia, Eastern Europe, Italy, Greece, Iran, the Middle East, Spain, North Africa, Argentina, Uruguay, Australia, New Zealand, and Ireland. In North America, the disease is seen mainly in Canada, Alaska, and the southwestern United States, particularly in New Mexico, Arizona, and Nevada.
Article: Echinococcus multilocularis Revisited. (2001)
INDEX
https://www.ajronline.org/doi/10.2214/ajr.176.5.1761207
American Journal of Roentgenology.
2001;176: 1207-1212. 10.2214/ajr.176.5.1761207
by Benedikt V. Czermak1, Karin M. Unsinn1, Thaddeus Gotwald1, Peter Waldenberger1,
Martin C. Freund1, Reto J. Bale1, Wolfgang Vogel2 and Werner R. Jaschke
Read More: https://www.ajronline.org/doi/10.2214/ajr.176.5.1761207
May 2001, Volume 176, Number 5
(This article has MANY photos of various scans)
E. granulosus cysts are characterized by typical radiologic patterns that are easily diagnosed, but diagnosis of E. multilocularis lesions is more difficult. The alveolar cysts grow by exogenous proliferation and behave like a malignant neoplasm. Therefore, E. multilocularis lesions can cause physicians to generate a long list of differential diagnoses, including malignant tumors. ...
We give an overview of the various radiologic patterns produced by E. multilocularis lesions as seen on sonography, CT, and MR imaging and discuss the involvement of various organs and tissues and common complications.
E. multilocularis is endemic in much of the upper Midwest of the United States, Alaska, Canada, Japan, central Europe, and parts of Russia. Definitive hosts are foxes and, less commonly, cats and dogs. Intermediate hosts are wild rodents. Humans are infested either by direct contact with definitive hosts or indirectly by intake of contaminated water or contaminated plants such as wild berries. E. multilocularis can affect any organ or tissue in the body, although the liver and the lungs are the most common sites of hydatid disease. ...
On sonography, these lesions usually show a �hailstorm pattern�.
This pattern represents the histopathologically heterogeneous stroma containing microscopic metacestodal vesicles, areas of nonliquefactive necrosis, entrapped host tissue, and microcalcifications, which account for the stroma's relatively increased echogenicity. ...
In advanced stages, peripheral calcifications may be seen within the areas of central necrosis. Secondary pyogenic infection may occur at any time during the course of disease, resulting in abscess formation. Apart from the typical peripheral irregular calcifications, large homogeneous), multiple punctiform, or scattered calcifications may be seen. Calcifications are found in 90% of all infected patients. ...
Hilar infiltration is observed in approximately 50% of all patients, resulting in dilatation of the intrahepatic bile ducts and invasion of the portal vein, the portal branches, and the hepatic veins. These conditions lead to hypoperfusion and subsequent atrophy of the affected liver segments). This atrophy is further aggravated by marked fibroinflammatory reactions of the liver tissue. ...
Involvement of the Musculoskeletal System and Soft Tissue
Clinical symptoms include thoracolumbar pain, abscess and fistula formation, and painless palpable nodules. In most patients, bone lesions develop as a result of progressive invasion of the adjacent echinococcal tissue into the bone. Therefore, the sternum and the vertebrae are the most common sites of osseous lesions. Lesions caused by hematogenous dissemination have been described in the ribs, vertebrae, and gluteal region.
Soft-tissue lesions are displayed clearly on MR imaging and CT. Multiple small, clustered cystic structures can be identified.
Involvement of the peritoneum occurs because of secondary infection caused by either cyst rupture or direct invasion from adjacent structures. Patients present with abdominal distention, meteorism (Tightness and distention of the abdomen as a result of internal gas under pressure in the peritoneal cavity or in the bowel), and constipation.
On CT, the omentum appears thickened by multiple thin-walled hypodense cysts resembling pseudomyxoma peritonei. Lesions of the same morphology can be found in the minor pelvis mimicking drop-metastases or primary urogenital tumors. However, ascites is often missing even in cases of extensive involvement of the peritoneal cavity. Pancreas, adrenal glands, and kidneys may be affected by direct spread of adjacent echinococcal tissue or by hematogenous metastases. Retroperitoneal lesions may infiltrate veins and enclose arteries.
Conclusion
E. multilocularis lesions are difficult to diagnose.
The frequent presence of clusters of microcalcifications (appearing in 90% of the patients) is of great value in establishing a positive diagnosis, especially if the patient has few clinical symptoms and no history suggesting exposure to E. multilocularis, such as residing in a rural area. In cases of extensive peritoneal or retroperitoneal involvement, contrast enhancement and ascites usually are missing.
Presented at the annual meeting of the Radiological Society of North America, Chicago, November 1999.
Article:
INDEX
Article:
INDEX
Testing: the immunochromatographic VIRapid� HYDATIDOSIS test (2015)
INDEX
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4427020/
by G�lden S�nmez Tamer, Devrim D�ndar, H�seyin Uzuner, and Canan Baydemir,
Med Sci Monit. 2015; 21: 1219�1222.
Echinococcosis in humans is a disease caused by the larvae of Echinococcus granulosus (E. granulosus) and Echinococcus multilocularis (E. multilocularis). Serological tests are valuable, especially in the clarification of unexplained clinical findings and imaging methods. For this reason,
- indirect hemagglutination (IHA),
- latex agglutination,
- immunoelectrophoresis,
- immunoblotting,
- immuno-enzymatic tests,
- indirect fluorescence antibody test (IFAT), and
- enzyme-linked immunosorbent assay (ELISA) are used.
The purpose of this study was to investigate the value of an immunochromatographic test (ICT) specific for E. granulosus antibodies in the diagnosis of echinococcosis.
The ability of test to give fast results without need for equipment, devices, and specific storage conditions is an advantage. This test may be used due to its advantages in endemic regions for screening and diagnostic purposes.
... In the diagnosis of cystic echinococcosis, hydatid cyst fluid and crude antigens have shown higher sensitivity compared to purified cyst fluid components. Indirect hemagglutination (IHA), latex agglutination, immunoelectrophoresis, immunoblotting, immuno-enzymatic tests, indirect fluorescence antibody test (IFAT), and enzyme-linked immunosorbent assay (ELISA) are used in serological diagnosis. However, these diagnostic methods require special tools and equipment.
The use of rapid diagnostic methods in the detection, isolation, identification, and count of pathogen factors in clinical, food, and environmental samples and their metabolites was first started in the 1960s. These tests are cheap, rapid, and have high specificity and sensitivity. Moreover, the test requires no special equipment for use and can be read by eye, and can be used by people who are not expert. This qualitative and semi-quantitative test detects antibody, antigen, and nucleic acid products. Its shelf-life can be increased up to 2 years by packaging inside a plastic cassette. The immunochromatographic VIRapid� HYDATIDOSIS (Vircell, Spain) test is a tape test that contains 5/B antigen of E. granulosus, works for serum and plasma samples, and gives legible and qualitative results within 30 min. ...
In the last 20 years there have been significant improvements on the serological diagnosis of echinococcosis. Sensitivity and specificity of the diagnostic tests were increased by use of new antigens and methods. Many serological tests were developed for the diagnosis of this disease. In this study, cystic echinococcosis-specific IgG type antibodies were studied with the immunochromatographic test. We found that it agrees with ELISA for specificity and sensitivity.
Sensitivity of the immunochromatographic test was 96.8%, its specificity was 87.5%, positive predictive value was 98.9%, and negative predictive value was 70%. Similar results were obtained in other studies. The highest performance was in active cysts in the serological diagnosis of echinococcosis. ...
.. camel hydatid cyst fluid was used as the antigen and 26 cystic echinococcosis patients and 35 patients with other parasitic infections were evaluated by this rapid test. Sensitivity of the test was detected as 100% and specificity as 91.4%. It was reported that this test was easy to use and gives results in 15 min. A similar result was obtained by rapid dot immunogold filtration assay (DIGFA) that gives the result in as fast as 3 min in the diagnosis of cystic and alveolar echinococcosis.
In this study, E. granulosus purified hydatid cyst fluid extract (Eg CF and AgB), crude antigens, E. granulosus protoscolex extract (EgP), and E. multilocularis metacestode antigen (Em2) were used. This is a rapid diagnostic method that is as easily read as the immunochromatographic test; its sensitivity is 80.7% in cystic echinococcosis and 92.9% in alveolar echinococcosis. ...
In our study, the immunochromatographic VIRapid� HYDATIDOSIS test was shown to work well in detecting antibodies against E. granulosus in human serum samples. It is important to have high specificity and sensitivity and high positive and negative predictive values for rapid diagnostic tests. However, in specificity studies among different parasitic diseases, antigenic similarities may be observed between Echinococcus and Taenia species. Therefore, the ICT test can also detect the antibody in taeniasis patient serum, which decreases its specificity. ...
Testing: Diagnostics in cystic echinococcosis: serology versus ultrasonography
INDEX
https://pubmed.ncbi.nlm.nih.gov/25254522/
by Johanna Wuestenberg, Beate Gruener, Suemeyra Oeztuerk, Richard A Mason,
Mark M Haenle, Tilmann Graeter, Atilla S Akinli, Peter Kern, Wolfgang Kratzer
Turk J Gastroenterol. 2014 Aug;25(4):398-404.
Cystic echinococcosis (CE) is the most widespread zoonosis worldwide.
The objective of the present study was to compare diagnostic methods in the work-up of suspected cystic echinococcosis of the liver.
Data from a total of 68 patients were compiled and analyzed.
Results:
A diagnosis of cystic echinococcosis was made in 36.8% of patients.
Broken down according to WHO criteria,
- patients with at least one echinococcus cyst were determined in 12.0% of cases to exhibit cysts consistent with stage 1 disease (CE1),
- while in 24.0%, cysts consistent with CE2 and CE3 were identified.
- CE4 and CE5 cysts were identified in 32.0% and 8.0% of patients, respectively.
- Solitary cysts were found in 60.0% of patients with cystic echinococcosis,
- while in patients with at least one cystic lesion, there were most often multiple cysts.
The indirect hemagglutination test (IHA) and echinococcus-specific immunoglobulin E (IgE) concentration showed a higher sensitivity (60.9%, 68.4%) than did the enzyme-linked immunosorbent assay (ELISA) for Echinococcus multilocularis (Em2+) and total IgE (11.1%, 38.9%). The respective specificities of all 4 serological methods lay between 83.9% and 88.9%.
Conclusion: (2014)
Our data show that ultrasound remains the diagnostic method of choice in the work-up of cystic lesions of the liver suspected to be due to Echinococcus granulosus. Serological methods can serve an adjunctive role.
Testing: ECHNO, Echinococcus Antibody, IgG, Serum Test. (2016)
INDEX
https://www.mayocliniclabs.com/test-catalog/Clinical+and+Interpretive/64985
LINK: Download Test.
https://www.mayocliniclabs.com/test-catalog/
download-setup.php?format=pdf&unit_code=64985
LINK: https://www.mayocliniclabs.com/
LINK: Microbiology Test Request (T244)
https://www.mayocliniclabs.com/it-mmfiles/Microbiology_Test_Request_Form.pdf
Fees
Authorized users can sign in to Test Prices for detailed fee information.
https://www.mayocliniclabs.com/customer-service/client-price-lookup/index.html
Clients without access to Test Prices can contact Customer Service 24 hours a day, 7 days a week.
Prospective clients should contact their Regional Manager.
For assistance, contact Customer Service.
Telephone: 800-533-1710 --- 507-266-5700
-- Email : mliintl@mayo.edu (International)
(No author or publication date provided)
RidaScreen Echinococcus IgG enzyme-linked immunosorbent assay (ELISA)
Useful For
Detection of antibodies to Echinococcus species, including Echinococcus multilocularis and Echinococcus granulosus
Clinical Information
Echinococcosis, also referred to as hydatidosis or hydatid disease, is 1 of the 17 neglected tropical diseases recognized by the World Health Organization and affects over 1 million people worldwide. Echinococcus species are tapeworms or cestodes, and 2 main species infect humans: Echinococcus granulosus and Echinococcus multilocularis.
With respect to geographic distribution, E granulosus can be found worldwide but, more frequently, is found in rural grazing areas where dogs may feed on infected sheep or cattle carcasses. E multilocularis is largely localized to the northern hemisphere. The definitive hosts for E granulosus are dogs or other canids, while the definitive host for E multilocularis are foxes and, to a much lesser extent, canids.
Echinococcus tapeworms reside in the small intestine of definitive hosts and release eggs that are passed in the feces and ingested by an intermediate host, typically sheep or cattle in the case of E granulosus or small rodents for E multilocularis. The eggs hatch in the small bowel, releasing an oncosphere that penetrates the intestinal wall and migrates through the circulatory system to various organs where it develops into a cyst that gradually enlarges producing protoscolicies and daughter cysts, which fill the interior. The definitive host becomes infected following ingestion of these infectious cysts. Humans become accidentally infected following ingestion of Echinococcus eggs.
In humans, E granulosus (cystic echinococcal disease) cysts typically develop in the lungs and liver, and the infection may remain silent or latent for years (5-20 years) prior to cyst enlargement and symptom manifestation.
Symptomatic manifestations include
- chest pain,
- hemoptysis, ( ) and
- cough for pulmonary involvement and
- abdominal pain and biliary duct obstruction for liver infection.
E multilocularis (alveolar echinococcal disease) infections manifest more rapidly than those of E granulosus and similarly to a rapidly growing, destructive tumor, resulting in abdominal pain and biliary obstruction.
Rupture of cysts can produce
- fever,
- urticaria, ( ) and
- anaphylactic shock.
Diagnosis of echinococcal infections relies on characteristic finding by ultrasound or other imaging techniques and serologic findings. Fine-needle aspirates of cystic fluid may be performed; however, they carry the risk of cyst puncture and fluid leakage, which may potentially lead to severe allergic reactions.
Importantly, infected individuals do not shed eggs in stool.
Cautions
Depending on cyst location, individuals may not develop high enough antibody titers to be detectable by serologic assays, leading to false-negative results. Cysts localized to the lungs, central nervous system or spleen, or cysts that are senescent, calcified, or dead are associated with lower serologic reactivity.
False-positive results may occur in patients with other helminth infections, including with Taenia species, Schistosoma species, and Strongyloides. Careful correlation with imaging findings and exposure history is required.
This assay may not detect antibodies to other species of Echinococcus, including Echinococcus vogeli and Echinococcus oligarthrus, both fairly uncommon causes of hydatid disease in humans.
Testing: LabCorp Burlington, NC, Echinococcus Antibody.
INDEX
https://www.labcorp.com/tests/138768/i-echinococcus-i-antibody
LabCorp Burlington
1447 York Court, Burlington, NC 27215-3361
Call LabCorp Support 24 hours a day (877)442-3226
For inquiries, the physician may contact Branch: 800-222-7566 --- Lab: 336-436-2762
LINK: Echinococcus-antibody test: USA $79.00
https://www.findlabtest.com/lab-test/infectious-disease-testing/
echinococcus-antibody-igg-eia-with-reflex-to-western-blot-quest-91307
Tapeworm (Echinococcus) IgG Test
Echinococcus Antibody (IgG), EIA with Reflex to Western Blot Lab Test procedure CPT Code: 86682
LINK: Lab Test Costs
https://www.findlabtest.com/lab-test/immunological-testing/
Recommend freezing serum.
To avoid delays in turnaround time when requesting multiple tests on frozen samples, please submit separate frozen specimens for each test requested.
Limitations
Antibody response is highly variable with respect to cyst location and individual response.
If a current infection is suspected, it is suggested that a convalescent serum sample be submitted in three to five weeks. All positive serology samples should be confirmed using a more specific test method (CDC) due to cross-reactivity with Taenia solium (cysticercosis).
CPT Statement/Profile Statement
The LOINC� codes are copyright � 1994-2021,
Regenstrief Institute, Inc. and the Logical Observation Identifiers Names and Codes (LOINC) Committee.
Permission is granted in perpetuity, without payment of license fees or royalties, to use, copy, or distribute the LOINC� codes for any commercial or non-commercial purpose, subject to the terms under the license agreement found at
LINK: https://loinc.org/license/
Additional information regarding LOINC� codes can be found at LOINC.org,
including the LOINC Manual, which can be downloaded at
LINK: LOINC.org/downloads/files/LOINCManual.pdf
Testing:
INDEX
Research: HPA (hypothalamic-pituitary-adrenal) axis.
INDEX
https://en.wikipedia.org/wiki/Hypothalamic%E2%80%93pituitary%E2%80%93adrenal_axis
5 April, 2020
LINK 2: https://adrenalfatiguesolution.com/hpa-axis/
HPA Axis Dysfunction
by Fawne Hansen,
2013-10-12
(includes an Infographic)
LINK 3: https://www.integrativepro.com/
Resources/Integrative-Blog/2016/The-HPA-Axis
10/31/2016 --- Lise Alschuler, ND
Program: https://go.integrativepro.com/hpa-axis-optimization-program.html
HPA AXIS OPTIMIZATION PROGRAM
Integrative Therapeutics
825 Challenger Drive
Green Bay, WI 54311 USA
LINK 4: https://www.wisegeek.com/
what-is-the-hypothalamic-pituitary-adrenal-axis.htm
Written By: Solomon Branch
Edited By: A. Joseph
Last Modified Date: 01 March 2020
LINK 5: https://www.sciencedirect.com/topics/
neuroscience/hypothalamic-pituitary-adrenal-axis
(Multiple articles spanning 2006 to 2019, summarized)
NOTE: The inhibition of the HPA (hypothalamic-pituitary-adrenal) axis is medically understood to be an antidote (to ???) that is provided by the drug/creme/lotion CLOBETASOL. This was prescribed for my use by a Lethbridge, Alberta physician for the treatment of Very ITCHY welts, rash, and white scabby skin manifestations commonly referred to in the medical field as Lichenization. One of the few known sources of this skin pathology is the presence of the Echinococcus multilocularis micro-tapeworm.
The HPA axis is a complicated set of relationships and signals that exist between the hypothalamus, the pituitary gland and the adrenals. This relationship is an absolutely indispensable part of our existence. It is dependent on the amount of cortisol in the blood, stress level and the wake/sleep cycle. If, for instance, the cortisol level gets too high, the hypothalamus and pituitary gland are stimulated and decrease their production of the hormones that began the process, thereby keeping the body in balance. The hypothalamic-pituitary-adrenal axis (HPA or HTPA axis) is also known as the
limbic-hypothalamic-pituitary-adrenal axis.
Constant stress of any kind can lead to dysfunction of the HPA axis.
In post-traumatic stress disorder there appears to be lower-than-normal cortisol release, and it is thought that a blunted hormonal response to stress may predispose a person to develop PTSD. Exposure to mild or moderate stressors early in life has been shown to enhance HPA regulation and promote a lifelong resilience to stress. In contrast, early-life exposure to extreme or prolonged stress can induce a hyper-reactive HPA Axis and may contribute to lifelong vulnerability to stress. ... the extreme stress of maternal separation, which disrupts the SHRP, may lead to permanent HPA dysregulation. A blunted ACTH response is common in depression. ... suicides and depressed patients generally showed evidence of over-activity of the HPA axis.
Many of the problems with which the HPA axis is involved are mood disorders, such as anxiety disorder, bipolar disorder, insomnia, posttraumatic stress disorder, borderline personality disorder, ADHD, major depressive disorder, burnout, chronic fatigue syndrome, fibromyalgia. Constant stress of the hypothalamic-pituitary-adrenal axis can also be a contributing factor to irritable bowel syndrome and alcoholism. Many of the mood disorders are treated with anti-depressants, which function by regulating the hypothalamic-pituitary-adrenal axis. Several monoamine neurotransmitters are important in regulating the HPA axis, especially dopamine, serotonin and norepinephrine (noradrenaline). There is evidence that an increase in oxytocin, resulting for instance from positive social interactions, acts to suppress the HPA axis and thereby counteracts stress, promoting positive health effects such as wound healing.
The H in HPA stands for Hypothalamus, a small part of the brain that does a very big job.
Its function is to send messages from the brain to the adrenals, the pituitary and other organs, so it is usually considered to be the starting point in the HPA axis. It is ultimately responsible for things like your circadian rhythm, your body temperature and your energy levels. (In other words) the hypothalamic-pituitary axis directly affects the functions of the thyroid gland, the adrenal gland, and the gonads, as well as influencing growth, milk production, and water balance. The hypothalamus is also involved in several important nonendocrine functions, such as temperature regulation, the activity of the autonomic nervous system, and control of appetite.
The anatomy and unique blood supply of the hypothalamic-pituitary axis are essential to its function.
The hypothalamic hormones are small peptides that are generally active only at the relatively high concentrations achieved in the pituitary portal blood system. Their small size and lack of known binding proteins results in rapid degradation and very low concentrations in the peripheral circulation. However, ectopic production of several of these hormones has been identified, both by normal white blood cells and by chromaffin cell tumors. Peripheral hormone receptors have also been identified, although their physiologic importance is not known.
The pituitary gland is even smaller than the hypothalamus, but it produces an extraordinary number of hormones that our bodies need. For example, this pea-sized gland produces vital hormones like Growth Hormone, Anti-Diuretic Hormone and Luteinizing Hormone. It is physically connected to the hypothalamus and sits at the base of the brain.
... the adrenal glands. We each have two of them, and they sit just above our kidneys.
Although physically separate from the hypothalamus and pituitary glands, they are deeply connected.
The adrenals produce even more hormones than the pituitary gland does � steroid hormones like cortisol, sex hormones like DHEA, and stress hormones like adrenaline and dopamine. The hormones produced by the adrenals control chemical reactions over large parts of our bodies. Cortisol is responsible for, among other things, slowing the immune system's inflammatory response and controlling blood pressure. High levels of cortisol result in a suppression of immune and inflammatory reactions. This helps to protect the organism from a lethal overactivation of the immune system, and minimizes tissue damage from inflammation.
... a typical response to a stressful situation.
(You are exposed to or perceive that there is a stressor ... something that raises fear, concern, anxiety, ... within you as a reaction to an identification of similarity to a stressful experience, trauma, educated/imprinted fear, or other expectation of danger or distress.)
... your hypothalamus releases corticotrophin-releasing factor hormone(CRF), which sends a message to the pituitary. This stimulates the pituitary�s ACTH (adrenocorticotropic hormone) production, which then prompts your adrenals to make cortisol. Among other things, cortisol raises the sugar in your bloodstream and prepares your body for the high-energy �fight-or-flight(-or pause)� response that it is anticipating. Your adrenals also release adrenaline, which raises your heart rate and increases your blood pressure.
These interactions continue until your hormones reach the levels that your body needs, and then a series of chemical reactions begins to switch them off. For example the cortisol released by the adrenals actually inhibits the hypothalamus and pituitary (so they stop sending signals to produce more cortisol!). This is just one of the automatic switches that we call negative feedback loops, and these loops are one reason why the HPA axis is so extraordinary.
With repeated exposure to stressors, the organism habituates to the stressor with repeated and sustained HPA axis activation. Therefore, it is important to support healthy cortisol levels in order to ensure the hypothalamus and pituitary glands maintain the appropriate level of sensitivity to the negative feedback of cortisol. Secretion of alarm chemicals such as epinephrine and norepinephrine from the adrenal medulla, as well as HPA axis activation persists along with the secretion of CRF, ACTH, and cortisol. Interestingly, with aging, the hypothalamus and pituitary are less sensitive to negative feedback from cortisol and both ACTH and cortisol levels (usually) rise as we age.
Some Feedback Loops.
Cortisol produced in the adrenal cortex will negatively feedback to inhibit both the hypothalamus and the pituitary gland. This reduces the secretion of CRH and vasopressin, and also directly reduces the cleavage of proopiomelanocortin (POMC) into ACTH and �-endorphins.
Epinephrine and norepinephrine (E/NE) are produced by the adrenal medulla through sympathetic stimulation and the local effects of cortisol (upregulation enzymes to make E/NE). E/NE will positively feedback to the pituitary and increase the breakdown of POMCs into ACTH and �-endorphins.
Release of corticotropin-releasing hormone (CRH) from the hypothalamus is influenced by stress, physical activity, illness, by blood levels of cortisol and by the sleep/wake cycle (circadian rhythm). In healthy individuals, cortisol rises rapidly after wakening, reaching a peak within 30�45 minutes. It then gradually falls over the day, rising again in late afternoon. Cortisol levels then fall in late evening, reaching a trough during the middle of the night. This corresponds to the rest-activity cycle of the organism. An abnormally flattened circadian cortisol cycle has been linked with chronic fatigue syndrome, insomnia and burnout. ...
During an immune response, proinflammatory cytokines (e.g. IL-1) are released into the peripheral circulation system and can pass through the blood brain barrier where they can interact with the brain and activate the HPA axis. Interactions between the proinflammatory cytokines and the brain can alter the metabolic activity of neurotransmitters and cause symptoms such as fatigue, depression, and mood changes.
Increased production of cortisol during stress results in an increased availability of glucose in order to facilitate fighting or fleeing (or, high awareness pausing). As well as directly increasing glucose availability, cortisol also suppresses the highly demanding metabolic processes of the immune system, resulting in further availability of glucose.
Glucocorticoids have many important functions, including modulation of stress reactions, but in excess they can be damaging. .... Deficiencies of the hippocampus may reduce the memory resources available to help a body formulate appropriate reactions to stress.
... paternal stress alters sperm miRNA content and reprograms offspring HPA axis.
In mammals, severe chronic stressors during critical periods of gestation have been shown to evoke elevated and prolonged glucocorticoid response in their offspring. Male offspring exposed to stress during early gestation displayed depressive �like� behavior and had an elevated stress response as measured by glucocorticoid levels after restraint stress. ... More recent work that utilized a mouse model in which the investigators had identified a period in early gestation when stress results in dysmasculinized and stress-sensitive male offspring demonstrated transmission of the stress-sensitive phenotype to the second-generation males. Micro RNA (miRNA) from the brains of these males showed a more female-like pattern.
Animal progeny of highly stressed dams during pregnancy were obese and showed impaired glucose tolerance as adults. In humans, maternal stressors such as daily social interactions, trauma, or exposure to natural disasters are associated with elevated basal cortisol levels as well as emotional or behavioral problems. Reduced cognition and risk of diseases such as autism and schizophrenia are increased in their children.
Symptoms: Possible indicators of infestation.
INDEX
CBC Radio --- Posted: Jun 07, 2019
https://www.cbc.ca/radio/asithappens/as-it-happens-friday-edition-1.5166570/
brain-surgeons-went-looking-for-a-tumour-but-found-a-tapeworm-instead-1.5166571
N.Y. neurosurgeon Jonathan Rasouli says the unexpected parasite
looked like a quail egg from the grocery store
Written by Sheena Goodyear.
Interview with Dr. Jonathan Rasouli produced by Allie Jaynes.
LINK 2:
https://www.healthline.com/health/echinococcus
Medically reviewed by -- Judi Marcin, MD on June 2, 2016
Written by MaryAnn DePietro
LINK 3: https://www.cdc.gov/parasites/echinococcosis/health_professionals/index.html
Page last reviewed: August 28, 2019
LINK 4: Echinococcosis.
https://www.cdc.gov/parasites/echinococcosis/gen_info/ae-faqs.html
Page last reviewed: December 12, 2012
LINK 5: Superinfection of a Dead Hepatic Echinococcal Cyst
with a Cutaneous Fistulization.
https://www.hindawi.com/journals/crira/2017/9393462/
Giuseppe Cicero , Alfredo Blandino , Giorgio Ascenti, Tommaso D�Angelo , Luciano Frosina,
Carmela Visalli, Ignazio Salamone, Maria Adele Marino, Marco Cavallaro, and Silvio Mazziotti
Case Reports in Radiology --- Volume 2017 |Article ID 9393462 | 5 pages
Additional LINK: https://doi.org/10.1155/2017/9393462
IMAGES noted can be observed in the original document at the above LINKS.
LINK 6: Cutaneous Disease as the First Manifestation of Cystic Echinococcosis.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4973166/
Virginia Velasco-Tirado, Manuela Yuste-Chaves, and Moncef Belhassen-Garc�a
Am J Trop Med Hyg. 2016 Aug 3; 95(2): 257�259.
SYMPTOMS:
- insomnia,
- nausea,
- vomiting,
- chest pain,
- trouble talking,
- generalized itching,
- nightmares,
- hallucinations,
- pain in one's shoulder,
- pain in one's abdomen,
- tenderness in one's ribs,
- hand or foot going numb,
- coughing up bloody mucus,
- erythematous (red) scaly skin areas,
- Pain or discomfort in the upper abdominal region.
- rupture of the cysts into the biliary tract,
- skin lichenification & hyperpigmentation,
- cystic rupture into the peritoneum, skin, digestive tract, or thorax,
- may mimic those of liver cancer and cirrhosis of the liver,
The cysts are mainly found in the liver and lungs but can also appear in the spleen, kidneys, heart, bone, and central nervous system, including the brain and eyes.
It takes a few months before symptoms appear.
Certain strains of the parasite can have a longer incubation period that may last up to a few years.
People with compromised immune systems are also more vulnerable to the disease
The infection is rarely diagnosed in North America.
It occurs more often in the Mediterranean, Middle East, Africa, and Central Asia.
If left untreated, the parasite can kill its human host in 10 to 15 years ...
Pain or discomfort in the upper abdominal region, weakness, and weight loss may occur as a result of the growing cysts.
Symptoms may mimic those of liver cancer and cirrhosis of the liver.
The infection affects the liver in about 75 percent of people who contract it.
Symptoms may include pain in your abdomen and the formation of cysts on your liver.
The infection affects the lungs in about 22 percent of people who contract it.
Respiratory symptoms may include chest pain and coughing up bloody mucus.
Other areas of your body can also be affected, including your skin, spleen, or kidneys.
Although the course of the liver hydatid disease is usually asymptomatic, complicated forms are not rare, occurring in 30�60% of the patients.
The main complications include traumatic or idiopathic rupture of the cysts into the biliary tract, which is the most frequent, or into peritoneum, skin, digestive tract, or thorax, due to a transdiaphragmatic involvement.
Large and superficial hepatic cysts are considered to be the most susceptible to break.
The removal of the tiny parasite marked the conclusion of a more than year-long ordeal for Rachel Palma, a 42-year-old newlywed from Middletown, N.Y.
She first went to the doctor in January 2018 with a laundry list of neurological symptoms, she told the Washington Post.
She couldn' t sleep, and when she did, she had nightmares. She was hallucinating.
She had trouble talking. She kept dropping things. Her right hand and the right side of her face were numb.
An MRI scan revealed a lesion in the frontal left lobe of her brain.
That, combined with her symptoms, led doctors to conclude she had a brain tumour.
The only thing left to do was open up her skull and determine whether it was malignant or benign.
Neither the doctors nor Palma know how she got the parasite, which is called 'Taenia solium and is extremely uncommon in North America."
Some people get it by ingesting microscopic tapeworm eggs found in raw or undercooked pork, or unwashed fruits and vegetables from overseas. But Palma has never travelled outside the U.S.
Persons with cystic echinococcosis often remain asymptomatic until hydatid cysts containing the larval parasites grow large enough to cause discomfort, pain, nausea, and vomiting. The cysts grow over the course of several years before reaching maturity and the rate at which symptoms appear typically depends on the location of the cyst. The cysts are mainly found in the liver and lungs but can also appear in the spleen, kidneys, heart, bone, and central nervous system, including the brain and eyes. Cyst rupture is most frequently caused by trauma and may cause mild to severe anaphylactic reactions, even death, as a result of the release of cystic fluid.
Alveolar echinococcosis (AE) is characterized by parasitic tumors in the liver and may spread to other organs including the lungs and brain. In humans, the larval forms of E. multilocularis do not fully mature into cysts but cause vesicles that invade and destroy surrounding tissues and cause discomfort or pain, weight loss, and malaise. AE can cause liver failure and death because of the spread into nearby tissues and, rarely, the brain. AE is a dangerous disease resulting in
a mortality rate between 50% and 75%, especially because most affected people live in remote locations and have poor health care.
A 61-year-old man from a rural area (Salamanca, Spain), who had contact with dogs, was admitted with generalized itching for 4 years. He was treated with oral antihistamines. A physical examination revealed greyish hyperpigmentation and severe lichenification and infiltration on the face, without mucosal pigmentation. His trunk and limbs showed xerosis, erythematous scaly skin areas with lichenification and hyperpigmentation.
Designating E. multilocularis infection as reportable in humans and animals is potentially important because, in AE-endemic areas (i.e., Europe), a large proportion of the economic burden associated with human AE is attributable to patients typically being diagnosed in the late stages of the disease, requiring lifelong chemotherapy and occasionally interventional procedures (e.g., percutaneous biliary and centroparasitic abscess drainage). Therefore, the ability to anticipate E. multilocularis exposure and to diagnose early-stage human AE is essential to reduce the need for long-term treatment, thereby minimizing the economic burden associated with the disease.
INDEX
INDEX
INDEX
Article: Lichens and People:
Uses, Benefits, and Potential Dangers.
INDEX
https://owlcation.com/stem/
Lichens-and-People-Surprising-Interesting-and-Helpful-Uses
by Linda Crampton
Updated on July 27, 2019
LINK 2: https://www.cbc.ca/news/technology/lichen-yeast-1.3689468
Lichens aren't quite what we thought, shocked scientists discover,
New yeasts found to be secret partners with known fungi and algae.
by Emily Chung � CBC News
Last Updated: July 22, 2016
What was eventually shared with me is that the term "lichenization" when applied to skin conditions in Medical descriptions or diagnoses only carries the meaning that the skin conditions APPEAR to look like lichens. There is NO direct association between the description and the reality of the skin condition having ANY connection to Lichens.
... Lichens have a wide variety of shapes and body forms.
They also have many possible colours, including black, grey, white, green, blue-grey, yellow, orange, red, and brown.
Despite their appearance, they aren't plants. Their body contains both a fungus and an alga. Each organism helps the other in some way, creating a beneficial partnership.
What Are Lichens?
Lichens are ... classified into three main types, based on the form of their body, or thallus.
Foliose types have a leaf-like appearance.
Fruticose types have a highly branched form. They may be erect or hanging.
Crustose types look like a crust that has formed on a surface.
Intermediate and unusual forms of lichens exist.
For example, scaly types look like a cross between a crustose form and a foliose form.
Jelly lichens live in moist areas and have a gelatinous appearance when wet.
Unlike a plant, a lichen doesn't have roots, stems, or leaves.
It's attached to its substrate by filaments called rhizines or by a single, central extension of the thallus called a holdfast. Most of the water and nutrients that the thallus needs are absorbed from the surrounding air and raindrops instead of through the rhizines or holdfast.
... Lichens perform useful functions in nature. They provide shelter for other organisms.
They also provide food for animals and materials that they can use to build their homes or nests.
When lichens grow on rocks, the chemicals that they release contribute to the slow process of rock breakdown and soil formation.
... In 2016, scientists made a surprising discovery.
They found that many lichens consist of a fungus, an alga or a cyanobacterium, and a yeast belonging to a group known as the basiodiomycetes. The presence of the yeast was unexpected. The researchers think that this organism makes chemicals that protect the lichen from microbes and predators. ...
... The new yeast has apparently gone undetected in lichens for more than a century, despite the fact that scientists all over the world have devoted entire careers to studying lichens closely with microscopes and genetic testing.
... It concerned two lichens that grow in B.C. and Montana and considered separate species for 100 years.
One called wila or edible horsehair lichen, also known by the scientific name Bryoria fremontii, is a brown-coloured lichen that was an important traditional food for many First Nations in northwestern North America.
The other, called tortured horsehair lichen or Bryoria tortuosa, is yellow and poisonous.
However, a recent genetic analysis showed that they were genetically identical � they were made up of exactly the same species of fungus and the same species of algae. ...
Traditional DNA analysis relies on probes or lures to fish out certain characteristic regions of genetic material, partly based on what scientists expect to find � like calling out names in a dark room to see who's there, (Toby) Spribille said.
Newer techniques instead look for all genes that are in the process of being translated into proteins via "messenger" molecules called RNA. (Toby) Spribille likens the technique to turning on the lights.
... the RNA they found came not just from the fungus and the alga known to be associated with the lichens, but ... a new kind of yeast, belonging to the taxonomic group Basidiomycota, the same one that button mushrooms belong to. ... Yeast cells and DNA were extremely common in the yellow, poisonous lichen, but rare in the edible brown lichen.
"Each lichen has a specific strain of the yeast," McCutcheon said.
"These form several new fungal families."
(John McCutcheon, a microbiologist at the University of Montana and
a research fellow with the Canadian Institute for Advanced Research)
DNA analysis suggests the yeast has been part of lichens for more than 100 million years � since the end of the Early Cretaceous, when dinosaurs like spinosaurus and allosaurus roamed the Earth, and flowering plants first appeared.
... Usnic acid has been found in several lichen species, ... Tests in laboratory equipment and lab animals show that usnic acid has antimicrobial properties and kills bacteria, fungi, and viruses. It also decreases inflammation and prevents some types of cancer cells from reproducing. Unfortunately, it may cause serious liver damage in humans. Clinical tests of the effectiveness of usnic acid in the human body are lacking. Substances may not have the same effect in our body as they do on isolated cells and inside lab animals.
The wolf lichen (Letharia vulpina) ... contains a yellow chemical called vulpinic acid, which is poisonous to mammals. ... Lab research shows that vulpinic acid can kill certain kinds of bacteria.
Ulla Kaasalainen from the University of Helsinki has discovered that 1 in 8 species of lichens wield microcystins, a group of poisons that cause liver damage in humans and other animals. These chemicals are manufactured by blue-green bacteria known as cyanobacteria.
� Ed Yong, Discover magazine
Some lichens are very tolerant to pollutants such as nitrogen and sulphur compounds, while others are very sensitive to the presence of one or both of these chemicals. ... Lichens have a high resistance to damage by dehydration and the ability to quickly absorb a large quantity of water after dehydration ends. ...The organisms stop photosynthesizing when they dry out and start producing food again as they absorb water.
Lichens absorb and store radioactive substances, such as cesium and strontium compounds, without apparent harm.
Their thalli can be tested for the presence of radioactive compounds in order to learn about their environment.
At least some species of lichen are very resistant to dangerous radiation.
In a 2005 experiment, 2 species spent 16 days in space inside an orbiting satellite. Here they were exposed to "massive" doses of ultraviolet and cosmic radiation. When they returned to Earth they had nearly the same photosynthetic ability as before the flight. In addition, most of the lichens' cells had no observable damage when examined under high magnification.
Treatment for Skin Lichenization.
INDEX
https://healthyfocus.org/home-remedies-for-lichen-sclerosus/
10 Home Remedies for Lichen Sclerosus
Publisher: https://www.facebook.com/.../healthyfocusorg/...
Medically Reviewed by Dr. Sumreen Anwar MBBS, B. Sc , M. Phil
Reviewed & Approved on October 27, 2018
Written by Marc Seward
Updated: 2019-07-03
LINK 2: https://www.davidwolfe.com/lichen-planus/
Lichen Planus Causes, Symptoms & 9 Natural Treatments
by David Avocado Wolfe
2017-11-30
Lichen sclerosus is a fairly rare condition characterized by white, patchy skin which is thinner than usual.
It is also sometimes called LS or White Spot Disease.
Both genders can be affected by lichen sclerosus and it can occur to people at any age.
The condition is not contagious.
This disease is (thought to be) triggered by the immune system in response to stress, allergens or a viral infection, or, may be caused by hormone problems, or, other yet to be determined factors. Hepatitis C is another risk factor. Research has found a statistically significant association between hepatitis C and lichen planus. Medications containing arsenic, bismuth, gold or quinidine have been implicated. These include antibiotics, diuretics, flu vaccines, medications for diabetes, malaria, high blood pressure and heart disease. Amalgam Fillings may ... leading to the development of oral lichen planus. Bone marrow transplant recipient and middle-aged adults are especially at risk.
It may affect the skin, scalp and nails, as well as the mouth and the genitals. There are various symptoms of lichen sclerosus including small white or shiny spots appearing on your skin. These small spots develop into larger plaques which become thinner and crinkled. Skin can tear more easily and there may be bleeding, blisters and itching.
4 Main Types of Lichen Planus
-
Reticular
This features a white web-like pattern that is easy to discern. The pattern is called �Wickham�s Striae.�
-
Erosive
Noted by the bright red rash that typically affects mucous membranes.
The mouth, gums, cheek, tongue, and genitals are especially prone. In more severe cases, ulceration can occur.
Most people experience moderate to severe discomfort while eating and drinking.
Common irritants include acidic and spicy foods. Extreme hot and extreme cold can worsen the pain.
-
Bullous
The fluid-filled blisters and lesions occur in the mouth, genitals, lower limbs and trunk.
-
Atrophic
The rarest form, it typically affects the trunk and legs.
The rash features whitish blue papules with a center that has atrophied or broken down.
Symptoms include the following.
- Itching which can range from moderate to severe.
- Pain and discomfort.
- Smooth white blotches on the skin.
- Wrinkled patches on the skin.
- Bleeding, blisters and ulcerated lesions in very severe cases.
- Skin more prone to tearing and bruising.
- Painful sexual intercourse.
- sleep disturbance,
- hypotension,
- loss of appetite,
- hypoglycemia,
- weight loss,
- tearfulness and
- irritability are also possible.
Treatments.
- may clear up spontaneously, if symptoms are not too severe.
-
Vitamin A
As lichen planus targets skin and mucous membranes, increasing your intake of vitamin A may help.
During an outbreak, eat more vitamin A rich foods.
These include raw carrots, sweet potatoes, kale, spinach and winter squash.
In addition to treating the rash, vitamin A supports the immune system and fights inflammation.
-
Oats
... oats as a gentle exfoliator and skin soother.
As the lesions and blisters transform through the course of the disease, a gentle exfoliation is a perfect treatment.
It allows you to rub off the dead skin to relieve itching, and improve the appearance.
For a simple oat exfoliation, here is a simple recipe.
You can mix equal parts oats and raw yogurt and let stand at room temperature for 20 minutes.
Then mix in � part raw honey. Use the mixture in generous quantities over the affected areas.
Allow the treatment to set for 10 to 15 minutes. Finally, rinse thoroughly with warm water, and pat dry.
-
Folate
One study found that 44 percent of patients with oral lichen planus were folate deficient. ...
People at risk for folate deficiency include those with liver disease and people on certain medications.
Those medications include diuretics and those used to treat diabetes.
Liver disease, diuretics and diabetes medications can increase your risk of developing lichens planus.
Therefore, eat folate rich foods from the legumes family. These include garbanzo beans, pinto beans and lentils, as well as beets, asparagus, and avocados.
-
Corticosteroid creams and ointments.
They are typically applied to the affected area every day to start off with and,
the treatments being reduced to a few times a week after a couple of weeks.
Prolonged use of corticosteroids can cause more damage to the skin and can actually cause it to thin even further.
-
Apple Cider Vinegar
Many people suffering from lichen sclerosus have experienced a great deal of success with apple cider vinegar.
Do not confuse this vinegar with your ordinary table vinegar.
Good quality apple cider vinegar contains a rich array of nutrition as well as antibacterial properties making it ideal to deal with a variety of skin conditions.
You can drink a few tablespoons of apple cider vinegar each day for general health purposes.
To treat your lichen sclerosus, simply wet a cotton ball in the vinegar and gently apply it to the affected area of your body a few times a day. Be careful, try a very small amount at first to ensure it does not burn.
-
Castor Oil
Many sufferers find it to be an excellent and soothing remedy.
It is also cheap and readily available making it an attractive option.
To get the best benefits from your Castor oil, follow these simple instructions.
Combine 3 or 4 tablespoons of Castor oil with a few drops of lavender essential oil and store it away in a jar.
When the mixture has taken on a paste-like consistency, it is ready to use.
Apply it to the affected areas daily and you should start feeling relief from itching and it should also help to heal your lesions.
-
Lavender Essential Oil
... It has a vast array of medicinal uses and is known to be one of the most gentle oils for your sensitive skin.
You can apply lavender oil undiluted but it is probably better to dilute it with a carrier oil like virgin coconut oil before you apply it. According to people who have used the remedy, it can have a very dramatic effect in a very short space of time. ...
-
Aloe Vera
... Make sure that you have pure Aloe vera gel of at least 99% and it can be applied to your genitals to ease your symptoms.
Simply apply around a 1/8th of a teaspoon of gel to the affected area of your skin several times a day to experience welcome relief and keep your itch at bay.
-
Borax
Borax powder is among the most talked about and popular remedies for sufferers of lichen sclerosus.
It is also a potentially effective remedy for oral lichen planus.
You can simply put a tablespoon or so of borax powder and an equal amount of baking soda in your tub and soak in it for 20 minutes or so.
Alternatively, you can take it internally.
Add a 1/8th teaspoon of borax and an equal amount of pink Himalayan salt to a liter or so of filtered water.
Drink the solution throughout the day in very small amounts of around 50 mils at a time.
Try getting through the drink before bedtime each day for 2 weeks and see if it has had a positive effect.
-
Baking Soda
Baking soda may also help relieve the soreness and itching associated with the condition.
You could simply try adding a tablespoon or so to your bath and just soaking in it.
Alternatively, put a tablespoon in a glass with around a third cup of clean water.
Sit down on the toilet and then pour the solution directly on the genital area.
-
Emu Oil
... its excellent anti-inflammatory and antioxidant properties. ...
You can apply this healing oil directly to the affected areas of your skin and massage it in several times daily.
According to research, it is well-absorbed and you only need apply a small amount to deal with a range of inflammatory skin conditions. ...
-
Coconut Oil
Good quality extra virgin coconut oil ... can provide soothing relief from the itching and burning you experience.
It can also be used in conjunction with corticosteroid treatment by acting as a barrier and allowing you to spread your steroid cream on thinner. For oral lichen planus, coconut oil pulling twice a day may improve the symptoms and provide relief. The process helps to detoxify your mouth by literally sucking out the toxins. Benefits include killing bad breath, soothing a dry mouth, reducing inflammation, and boosting the immune system.
-
Magnesium
Studies ... have revealed that a magnesium deficiency could be linked chronic inflammatory stress.
According to recent estimates, some 60% of the adults in the US do not consume sufficient magnesium which can lead to a number of health problems. ...
-
Tea Tree Oil
... If you have oral lichen planus, a tea tree oil based mouthwash may aid in the healing, particularly with erosive and bullous types. However, some may find it further irritates the mouth. In this case, discontinue use immediately. When treating lichen planus on the scalp, mix tea tree oil, coconut oil, aloe vera, apple cider vinegar and raw honey. These substances have antibacterial, antifungal and antiviral properties. Together, rubbing them on the scalp can work to relieve the itching commonly associated with this condition.
-
Turmeric
Turmeric may be beneficial in changing the appearance and discomfort in oral lichen planus.
... the anti-inflammatory, antiviral and antibacterial properties of curcumin ... can actually inhibit the growth of squamous cell carcinoma of the head and neck. This type of carcinoma is a recognized risk of oral lichen planus.
-
Epsom Salt Baths
Epsom salt can provide relief by relieving sore muscles and detoxing the body.
It is known for helping to reduce stress, eliminate toxins and reduce pain and inflammation.
Prepare a warm bath, and add 2 cups of Epsom salt, stirring it around with your arm.
Soak at least 30 minutes for best results. Also, the addition of your favorite essential oils can provide additional relief.
-
Dietary Changes
Lichen sclerosus may be linked to the things that you eat so carefully monitoring your diet may be crucial.
One of the best diets that you can follow to keep your symptoms in check is the Candida diet, probiotics are also helpful.
Many of those who suffer from the condition also suffer from yeast infections and thrush so the Candida diet makes a lot of sense. You will need to cut refined sugars, processed dairy products and possibly even gluten and wheat from your diet. Try eating ... plenty of fermented foods like kefir, sauerkraut, and yogurt. Regular probiotic supplements can also play a positive role in eliminating yeast infections
It is relevant to note that MANY of these individual treatments are SUGGESTED as constructive while there is few reports of their use being Effective for some or many patients. Too often, both on the Internet in general, and, in research articles, suggested treatments are put forward with the rationalization that they SHOULD work. "Shoulds" often turn out to be wrong as often as 50% of the time.
Product: Creme Complete, Perrin Naturals.
INDEX
https://www.perrinnaturals.com/content/natural-treatment-lichen-sclerosus
US $47.99 --- 2 oz --- 2020-03-15
1-731-989-8388, M-F, 9-5 CDT
International shipping costs are approximately $15.50 USD for one-two items and gradually increases with more items.
Distributors located in Canada, UK, Australia, New Zealand, Sweden
https://www.perrinnaturals.com/outside-us
Natural Healing Clinic
470 8th Street South East
Medicine Hat, Alberta T1A1L9
Phone: 403-526-5700
Gaudaur Natural Foods
17 Andrew St N
Orilia, ON L3V 5H9
Phone: 705 325 7143
Toll Free: 1 800 819 8837
info@gaudaur.com
LINK: https://www.gaudaur.com/perrin-naturals/
A restorative, antioxidant, anti-viral, anti-bacterial, anti-yeast, moisturizing cream.
Ingredients:
Organic aloe vera, grape seed oil, organic beeswax, organic vegetable glycerin, organic cocoa butter, natural vitamin E in soy oil, organic castor oil, vegetable derived emulsifying wax, almond oil, organic safflower oil, organic extra virgin olive oil, honey, lavender oil, organic lecithin, vitamin C, n-acetyl cysteine, resveratrol, alpha lipoic acid, sodium bicarbonate, grape seed extract, coQ10, biotin, vitamin A & D, lemon oil, frankincense oil, peppermint oil, geranium oil, organic cornstarch, cream of tartar.
Ingredient Benefits
Aloe Vera to calm inflammation.
Resveratrol to encourage healthy skin growth.
Vitamin C to fight infection and act as an antioxidant.
Grape seed oil for it's high content of linoleic acid, an essential fatty acid essential for healthy skin.
Essential Oils for their therapeutic and antimicorbial activity to fight bacteria, fungus, and yeast infections
Grape Seed Extract for it's high content of polypheols that encourage healthy skin growth.
Vitamin E because it's been shown time and time again to be beneficial for the skin health.
Alpha Lipoic Acid and CoQ10 are two essential antioxidants found naturally in our skin,
and with their slow depletion need to be restored as we age.
Suggestions from Judy Perrin, Co-founder of Perrin Naturals
Possibly the strongest attack against the disease, Perrin�s Blend, is a sticky ointment.
By far it contains the highest concentration of the antioxidants Vitamin C, Alpha Lipoic Acid, and N-Acetyl Cysteine (NAC) and Grape Seed Extract, and Honey than any of our other products. For this reason it is possibly the most aggressive against Lichen Sclerosis (LS), yet if person is very raw and irritated, Perrin's Blend might be too harsh to start with because of the burning it might cause.
If ordering only one product for LS, I suggest starting with Creme Complete, our moisturizing cream highest in antioxidant concentration (excluding the Perrin�s Blend) and also diversity, containing CoQ10 and Resveratrol. Although it might also burn, it would be less intense.
Some who have been severely irritated have begun with Nutra Cream, our mildest cream, for a few days before even beginning with Creme Complete. Nutra Cream, although higher in grape-seed extract than Cr�me Complete, contains less of the burning antioxidants, such as Vitamin C and NAC. It is a thicker cream, thereby creating more of a protective shield against urination stinging and itching. ...
Even though our products don't usually burn on any other skin areas, almost any thing used in such a delicate area might cause burning. Most customers tell us that the burning subsides within 10-20 minutes and then they experience relief. Some have reported that after a few days it doesn't burn anymore. We have received only two reports of the products being too intense that they had to stop use. ...
Many order two products to start with - Perrin�s Blend and Cream Complete - beginning first with Creme Complete, using it for a few days before introducing Perrin's Blend. If ordering these two together, be sure to scroll down to the online store to get the combination special price.
Some include Nutra Cream in their order and begin with it (depending on the degree of initial irritation).
If ordering all three products, I suggest starting with Nutra Cream � it can be used anytime relief is needed � to hopefully help with rawness and irritation. Within 24-48 hours start applying Cr�me Complete up to 4 times daily for several days, especially applying well at bedtime before graduating to Perrin�s Blend. Then start using Perrin�s Blend at night.
Perrin's Blend, being in a base or raw honey, is a sticky ointment and would probably be uncomfortable for day use.
It also stains fabrics. ...
Although Creme Complete and Nutra Cream both contain some honey, they are spreadable creams for overall use while Perrin's Blend was designed for use in a small area (such as a lesion) and is hard to spread. It is thick and might need to be thinned by adding a small amount of pure honey for spreading over such a tender area for LS. A pad may be needed because of the staining.
Your order selection should depend on the extent of your condition and how aggressively you want to start.
Because everyone is different we know that nothing (not even a prescribed medicines) always work the same for everyone and that no one has a magic formula that brings the same successful results for every single person, yet we are grateful to receive so many positive reports from people being helped. Hopefully this information will help you decide what you need and you, too, can find relief from this disease.
Judy Perrin
Products: Taro-Clobetasol Cream.
INDEX
https://content.medicineshoppe.com/clobetasol
LINK 2: https://www.drugs.com/mtm/clobetasol-topical.html
LINK 3: https://pubchem.ncbi.nlm.nih.gov/compound/clobetasol
2020-04-11
Clobetasol treats inflammation and itching caused by skin conditions such as psoriasis.
Do not cover treated skin areas with a bandage or other covering unless your doctor has told you to.
Clobetasol topical (for the skin) is used to treat inflammation and itching caused by plaque psoriasis or skin conditions that respond to steroid medication.
Uses of Clobetasol
- Dermatitis
- Facial Dermatoses
- Foot Dermatoses
- Hand Dermatoses
- Inflammation
- Leg Dermatoses
- Scalp Dermatoses
Clobetasol Brand Names
- Clobevate
- Clobex
- Cormax
- Embeline
- Impoyz
- Isovate
- Olux
- Temovate
Clobetasol is part of the drug class: Corticosteroids, very potent group IV
Steroid medicines can increase the glucose (sugar) levels in your blood or urine.
Tell your doctor if you have diabetes.
Apply a thin layer of medicine to the affected skin and rub it in gently.
Do not apply this medicine over a large area of skin unless your doctor has told you to.
Avoid applying clobetasol topical to your face, underarms, or groin area.
If you use clobetasol to treat plaque psoriasis, you should stop using the medicine once your skin symptoms are controlled.
This medicine is for short-term use only (2 weeks, or up to 4 weeks for scalp psoriasis).
Clobetasol topical side effects
Get emergency medical help if you have signs of an allergic reaction:
- hives;
- difficult breathing;
- swelling of your face, lips, tongue, or throat.
Call your doctor at once if you have:
- worsening of your skin condition;
- redness,
- warmth,
- swelling,
- oozing, or
- severe irritation of any treated skin;
- blurred vision,
- tunnel vision,
- eye pain, or
- seeing halos around lights;
- high blood sugar--
- increased thirst,
- increased urination,
- dry mouth,
- fruity breath odor; or
-
possible signs of absorbing this medicine through your skin
weight gain in your face and shoulders,
- slow wound healing,
- skin discoloration,
- thinning skin,
- increased body hair,
- tiredness,
- mood changes,
- menstrual changes,
- sexual changes.
Common side effects may include:
- headache
- burning,
- itching,
- troubled breathing
- unusual tiredness or weakness
- acne;
- irritability
- nausea
- swelling,
- sweating
- irritation of treated skin;
- dry or cracking skin;
- spider veins;
- stretch marks,
- thinning skin;
- rash or hives;
- thinning of the hair
- temporary hair loss
- pain in hairy areas,
- pus at the root of the hair
- facial hair growth in females
- redness or crusting around your hair follicles;
- Backache
- blindness
- blurred vision
- change in vision
- eye pain
- dry mouth
- fractures
- fruit-like breath odor
- increased hunger
- increased thirst
- increased urination
- loss of sexual desire or ability
- menstrual irregularities
- muscle wasting
- redness and scaling around the mouth
- stomach pain
- sugar in the urine
- tearing
- unexplained weight loss
- vomiting
2009 -- Like other topical corticosteroids, clobetasol propionate has anti-inflammatory, antipruritic, and vasoconstrictive properties. The mechanism of the anti-inflammatory activity of the topical steroids, in general, is unclear.
Clobetasol propionate preparations are some of the most potent topical corticosteroid preparations currently available. Because of its potency, the drug can suppress the hypothalamic-pituitary-adrenal (HPA) axis following topical application, and HPA-axis suppression has occurred following topical dosages as low as 2 g of the 0.05% ointment or cream (1 mg of clobetasol propionate total) or 7 g of the 0.05% foam (3.5 mg of clobetasol propionate total) daily.
Some data indicate that clobetasol propionate 0.05% lotion may be associated with a higher incidence of HPA axis suppression than clobetasol propionate 0.05% emollient cream. Because of the drug's potency and potential for causing adverse systemic effects during topical therapy, the usual dosage should not be exceeded, and occlusive dressings (including bandages) should not be applied to areas of clobetasol propionate application.
... corticosteroids are thought to act by the induction of phospholipase A2 inhibitory proteins, collectively called lipocortins. It is postulated that these proteins control the biosynthesis of potent mediators of inflammation such as prostaglandins and leukotrienes by inhibiting the release of their common precursor, arachidonic acid. Arachidonic acid is released from membrane phospholipids by phospholipase A2.
A group of CORTICOSTEROIDS that affect carbohydrate metabolism (GLUCONEOGENESIS, liver glycogen deposition, elevation of BLOOD SUGAR), inhibit ADRENOCORTICOTROPIC HORMONE secretion, and possess pronounced anti-inflammatory activity.
They also play a role in fat and protein metabolism, maintenance of arterial blood pressure, alteration of the connective tissue response to injury, reduction in the number of circulating lymphocytes, and functioning of the central nervous system.
INDEX
INDEX
Testing: Why Echinococcus multilocularis is usually NOT found.
INDEX
At present, 2021,
50% of cases are reportedly found in autopsies, and,
50% are found during surgery for a misdiagnosis.
WHY?!
There are 7 straightforward reasons for this diagnostic failure.
-
Patient Ignorance.
Few patients have heard of such a pathogen or know anyone who has been successfully diagnosed with it.
With the typically authoritarian structure of North American (Canada and the USA) medical institutions, employment and financing ... patients are imprinted with an expectation that their doctor should either know everything about medicine, or, have access to medical references, devices, and other personnel who can fill any gaps in their knowledge and bridge any deficiencies in their training or experience.
This has resulted in an attitude and expectation within most patients of passive ignorance about their health and that of others. In addition, mass media stereotypes, particularly American ones, emphasise this valuation of medical doctors as heroes, saviors, miracle workers, and, professionals. It is rare that patients have the personal enthusiasm and have developed the research skills necessary for an informed view of health dynamics and an openness of mind to that of continual learning. Echinococcus multilocularis is not a highly socially and media visible pathogen. Many thousands will die mysterious deaths before any interest is shown.
-
Symptom confusion.
With the exception of Skin Lichenization, which is not always an indicator, the other symptoms are often temporary, not acute, and often suggest the possibility of radically different health difficulties. Any instance of Echinococcus multilocularis may harbor a few similar symptoms yet result in others which may seem temporary, and may widen any concept of a pattern of symptoms. Increasingly in more recent years, a simplification of diagnostic assessments minimized to a projected possibility from not more than ONE symptom per visit, results in a prescription for a specific ailment when a symptom relates to as many as 16 widely divergent illness conditions. Co-morbidities increasingly present in patients in whom pathogens and toxicities have existed for decades and which the accepted norm of treatment has been to deaden and hide the symptom and never determine what the originating factor or factors might be and seek to resolve those. The political management want LOW cost.
The governing medical Associations want their professionals to deliver the best service with the minimum of time and resources ... essentially transforming them to technicians who follow routines. Doctors who remain in service in Canada must accept that they are best equipped and trained to provide the most relevant patient service, only, for the most acute of health problems. Anything further is conveniently addressed by minimizing the multivariable chronic problem into a simplistic acute urgency. Echinococcus multilocularis becomes urgent when the patient is on the autopsy table or in the grave.
-
Authoritarian attitude of elitism over patient interaction.
Most physicians in the "Western" economic and political nations have been taught, rewarded, and peer imprinted to evidence a pride and confidence in their abilities and sanctioned titles and privileges. Those who have sought to train additionally in other modalities, such as acupuncture or herbology ... have usually been ridiculed, avoided, and even penalized by the medical associations which are to represent them and focus on enhancing the health of patients. In addition, they often find themselves ostracised by peers and receiving little support from a patient community which is ignorant of new-to-them modalities ... and wanting to remain closed-minded.
With this attitude, honest, humble, and cooperative communication is discarded or avoided in exchange for one-sided, prejudiced, and demeaning styles verging on bullying, and, open to misinterpretations and misunderstandings. Significant diagnostic and prescribing errors have been reported by the medical Associations as frequent, for decades. Diagnosing possibilities for Echinococcus multilocularis in the Province of Alberta, and likely many other provinces, remains unlikely when most physicians and patients are unaware of it as a possibility, when a concern of the possibility is expressed by a patient and minimized or goes unheard by the doctor, and when accepted and promoted diagnosing procedures are most likely to miss it.
-
Diagnosis by Superstition.
Most doctors won't admit it, yet the reality of their prescribing is seldom beyond the simplicity of superstition.
They hear a symptom and immediately directly associate it with something they have read or been told in their training, and/or, heard from a fellow doctor, and/or, found was relevant for another patient. As there is never any followup with a patient, in my experience of over 70 years across 3 provinces, ... assuming that a patient had a positive result from a prescription because they did not return is fraught with many problems. If the prescription was fatal, the patient is not returning. If the patient did not take the drugs, which has been frequently noted as being as high as 40% of the time across decades ... the positive result may be that they did NOT take it.
Limiting the patient feedback about their health concerns to the statement of only ONE symptom when most sicknesses evidence at least several, and, when a multiplicity of symptoms may assist in narrowing down the possibilities ... again encourages errors, delays in relevant treatment, further declines in health, and, unnecessary fatalities. Most, if not all, of the known instances of Echinococcus multilocularis in Canada have followed YEARS of misdiagnoses and irrelevant treatments which served to simply increase the severity of the medical complications being experienced by the patient.
-
Misapplication of testing devices and irrelevant image assessments.
In all but the simplest of medical problems presenting dramatic indications, the use of much of the medical technology available in North America is skewed to keep institutional costs and political budgets low, and, miss medical problems which are more complex to diagnose and treat as well as those best served by surgical intervention. Ultrasounds, CT scans and MRI's are least costly when they are done quickly ... which requires a LOW resolution setting. These settings frequently make the discernment of non-calciferous masses difficult to impossible, regardless of their size. Even if they are detected, the low resolution reality makes pre-surgical assessment vague, and, guesswork.
This helps explain why a grapefruit sized sac filled with tapeworm eggs was missed until the patient was surgically opened and explored. Short of very specific and expertly assessed blood tests followed by an expert assessment of a HIGH resolution scan, instances of Echinococcus multilocularis often go undiagnosed until discovered in an autopsy, if the medical examiner is familiar with the parasitic manifestation, is politically allowed to report it, and if an autopsy is done. In the Province of Alberta, an autopsy is NOT done unless the victim is NOT under a doctor's care, and, the death appears to have been possibly the result of a criminal act.
-
Lack of Awareness in the Medical community.
Echinococcus multilocularis is almost unknown to Canadian and American physicians.
The Alberta Health website page on it minimizes knowledge of it as important on the basis that few cases have been diagnosed. This is akin to stating that COVID-19 is unimportant if we have few diagnosed cases while we test no one for it, know hardly what to look for, and, use diagnostic procedures almost guaranteeing that we miss it regardless of how common it is and regardless of whether a patient is before their technician doctor with it.
-
Provincial Autopsy Restrictions.
In the province of Alberta, Canada, autopsies are NOT performed on corpses of individual who have been under a doctor's care or have had a Family Doctor. In these cases an autopsy must be requested by family members BEFORE the body is disposed of, and, PAID FOR BY the family ($3,000 or more). Autopsies or performed in many North American centers by Medical Examiners and not by Coroners, after the many reports of fraudulent and incompetently performed autopsies in the early 2000's by coroners who had NO medical training or experience. Often, Medical Examiners are charged with determining simply if the death was caused by criminal or "natural" factors. Proceeding further in so-called "natural" cases to determine WHAT caused the death may often be avoided due to possible time and cost concerns.
Straightforwardly, this policy protects Family Physicians and other medical personnel from any responsibility in those cases where incompetence, denial, and errors have been made. This prevents such personnel (and the medical industry and services) from ever learning from any errors, sanctions incompetency, encourages denial, and minimizes statistics of occurrence and awareness. How many other provinces and states have similar restrictions.
A less straightforward reason is the dynamics of the parasite itself.
It is a microscopic tapeworm compared to that of more commonly known tapeworms.
Unlike most other parasites infecting the human body, its eggs never mature within the body.
Encountering an egg mass of almost any parasite within the human body is quite unusual.
Technical: Patient DI/Lab Results Report, 2020-11-26
INDEX
Received in printed format.
QUOTED for CT, Chest X-ray, Ultrasound, and Bili Hida Scans
All results performed dates from 2020 Nov 13/26
Images are not diagnostic.
Higher quality images are available in eroviewer and Impax
Technical: Impax Viewer.
INDEX
https://www.carilionclinic.org/sites/default/
files/2017-08/Impax%20User%20Guide.pdf --- 18 pages
Agfa Impax A Picture Archiving and Communication System (PACS)
Quick Reference Guide
LINK 2: VA Technical Reference Model v 20.10
https://www.oit.va.gov/Services/TRM/ToolPage.aspx?tid=5628
USA Dept of Veteran's Affairs
08/26/2020
This technology is not portable as it runs only on Windows platforms.
LINK 3: IMPAX Client Installation.
http://impaxupdater.palmettohealth.org/clientinstaller/en/
Microsoft .NET Framework 4.6.1 is also required.
LINK 4: agfa impax cd viewer.
https://www.updatestar.com/en/topic/agfa%20impax%20cd%20viewer
Searches for same and similar viewers with Download LINKS.
12/03/2020
LINK 5: https://impax.tech/about-us
You Impax Userid and Password are the same as your EPIC account.
You may hear it referred to as your Active Directory Account or AD account
LINK 6: Free DICOM Viewer for Windows.
https://dicom-viewer.en.softonic.com/
Innovation and Modernization Patuxent River (IMPAX)
As a Partnership Intermediary Agreement between the Naval Air Warfare Center Aircraft Division (NAWCAD) and the Georgia Tech Research Institute (GTRI), IMPAX has the ability to communicate directly with government agencies, industry, academia, and the public to assist with completing complex technological projects at a faster rate, with higher returns.
IMPAX is a picture archiving and communication system (PACS) solution.
IMPAX is a proprietary software for use at medical facilities using a digital radiology imaging system and supporting both local and remote access. The software allows clinicians to enhance their workflow through various image and communication functions. The client can connect to the PACS server from across office locations via thin and fat client technology.
Data is stored on the IMPAX Database Server which is compatible with Oracle Database or Microsoft Structured Query Language (SQL) Server database. The IMPAX Database Server stores the central database used by all components in the cluster and maintains a record of all database transactions in transaction log files.
The IMPAX Client software is used to view, interpret, and distribute medical reports and images.
The IMPAX Client installation program installs the full Client, excluding any integrated applications (such as TalkStation, IMPAX Reporting, Volume Viewing, the Orthopaedic application, or other clinical applications). To install it, you must be logged in as a Windows administrator.
The IMPAX Client focuses on the integration of PACS, RIS, and Reporting applications into a single delivery of information. A single IMPAX Client application can be used by a range of users on any appropriate, networked workstation they have access to.
Impax is set to log a user off the system after 20 minutes of inactivity.
If a user leaves the work-station for a long period of time, or if the workstation is simply idle for a while, IMPAX shuts down and returns to the Login screen
From the List AreaList AreaList AreaList Area, you can do a simple search for a study by Patient name, Patient ID, Accession Number, Study Date or Modality.
Select the desired study from your search results. The selected study highlights.
Double-clicking the desired study opens the Image Area Image Area Image Area Image Area with the image(s) as well.
From the TOP Toolbar at the top of the display screen,
Select the Window Level Window Level Window Level Window Level tool.
Using the mouse, click once on the image.
Move the mouse up and down and left to right to adjust the window level.
Click once on the Image again to set the window/level
---- Hint: Moving the mouse vertically (up and down) adjusts the brightness of the window/level.
---- Moving the mouse horizontally (right and left) adjusts the contrast of the window/level.
Impax�s Geometry tools allow users to change the orientation of the images.
Images can be rotated and flipped vertically and horizontally.
After selecting the Zoom Drop-down Tool from the Top of display toolbar ..
Increase or decrease the magnification in the Magnify Glass window, use the mouse scroll wheel.
Or Use the Page up or Page down keys on the keyboard.
To resize the Magnify Glass window, place the cursor over any part of the frame.
A double-arrow displays. Click and drag the window frame to a desired size.
It is important to close images as you are done viewing them.
Impax remembers what Studies are left open in the Image Viewing Area and will open them the next time you login in to Impax. Leaving images open in the viewing are will slow the login process for your next session because images must load in order for you to per-form your next search.
Free DICOM Viewer.
Anyone in the field of medicine knows the importance of DICOM.
An acronym for Digital Imaging and Communications in Medicine,
DICOM is a standard for medical imaging which allows users to store, print, and share data.
However, viewing one is not something you can easily do, as the usual image viewers do not support such a file.
You need to have a separate application to do such a task.
Free DICOM Viewer is one of those programs that can view DICOM files.
It is one of the better-known health applications that have several useful features.
If you want to access DICOM files and garner information about any disease, this app is worth a try.
DICOM represents the universal and fundamental standard in digital medical imaging.
It provides all the needed tools to represent and process diagnostically-accurate medical imaging data.
Contrary to popular opinion, DICOM is not just an image or file format.
It is an all-encompassing data transfer, storage, and display protocol designed and built to cover all functional aspects of digital medical imaging. This is why many view DICOM as a set of standards, rather than a single standard.
Media Freeware�s Free DICOM Viewer is an ideal choice when you want to view DICOM images.
The app comes with an interface that is easy to use, even by a novice user.
Its comprehensive set of functions�like zoom, rotate, and color change --- are laid out simply in the window.
Parameters, such as width and image size, are also adjustable.
The angle in which you can see the image is flexible, as well, and can be modified within the interface itself.
Free DICOM Viewer also allows the users to tag the image and reset it according to individual requirements.
It also lets the users manage the files easily since settings such as lighting can be adjusted.
Free DICOM Viewer supports quite a few formats, including PNG and JPEG.
It is a small-sized tool that requires less disk space. Moreover, its response time is very impressive, with little to no chances of crashing or freezing.
Technical: Zeroviewer.
INDEX
https://morton.co.za/xeroviewer/
LINK 2: XERO� Viewer.
https://www.agfahealthcare.com/he/usa/en/
binaries/XERO%20sheet%202013_tcm561-113934.pdf --- 2 pages
LINK 3: Quick Start Guide. 11 page pdf
Morton and Partners, Radiologists
https://morton-web.s3.amazonaws.com/XERO%20Final.pdf
(021) 276 2019 --- support@morton.co.za
Business Hours: 07:00-17:30
Afterhours (emergency) number: (083) 607-4613
Agfa HealthCare Corp.
10 S. Academy Street
Greenville, SC 29601 USA
Agfa and the Agfa rhombus are trademarks of Agfa-Gevaert N.V., Belgium, or its affiliates.
IMPAX, XERO, and ICIS are trademarks of Agfa HealthCare NV, Belgium or its affiliates.
XERO is a web-based medical imaging service intended for use by all our referring physicians or healthcare professionals. It provides access to radiology images and reports.
XERO enables authenticated users to search for and display available patient studies (reports and images) using a browser on a PC or mobile device. XERO is designed for reviewing medical imaging studies, and not for primary diagnosis.
Access XERO Viewer by going to https://mobile.morton.co.za/ and using your login details to access the patient�s information.
If you have not yet accessed XERO before, please contact our PACS support centre to help register your profile.
Contact them on: (021) 276 2019 or imaging@morton.co.za
System Preferences:
Xero Viewer is a web-based imaging platform and is thus system agnostic (i.e. will work on Windows, MacOS, iOS and Android).
Our IT team recommends using Chrome to access XERO for an optimal user experience.
In the delivery of care today, health systems around the world find themselves struggling to identify and dissemi-nate medical images data from various departments and dif-ferent locations to the caregivers who need that data. As the use of images grow, so does the challenge of providing all care providers have access to images. Yet, as more depart-ments generate imaging data and more providers value its use in patient care, simply consolidating storage does not solve the problem.
Based on innovative, no-application download technology, Agfa HealthCare�s XERO enterprise imaging viewer is a tech-nological breakthrough that allows any clinical user to view patient images, regardless of department or region of origin, at any time from any web-enabled device.
Any clinician can now request, and quickly receive, the images from multiple sources within a single, patient-centric view. It doesn't matter where the images are, or what ven-dor�s solution is hosting them. XEROVERSE, Agfa�s new multi-source discover technology will combine them all, in an instant, into one view. XERO is multi-patient ID domain capable.
XERO allows fast, secure viewing of all images and reports with no client software to install.
The AJAX-based technology works over net-works with a modest bandwidth, inside or outside the hospital, and on many popular browsers � virtually eliminating desktop maintenance costs while providing secure, efficient, and ubiquitous access to medical images and reports throughout the healthcare enterprise.
The PATIENT ID field is Morton & Partner's QP number and not the patient's ID number.
The format should be: QP-123456
Do not enter more than 2 fields in the search fields, as it slows down the search request.
The OFFLINE button reflects your CHAT STATUS with other users and not the system status.
The icon will change to ONLINE (green) if you are able to use this function.
Technical: NM Biliary HIDA Scan.
INDEX
What you should know about the HIDA scan.
https://www.medicalnewstoday.com/articles/320496
Medically reviewed by Suzanne Falck, M.D., FACP
Written by Jayne Leonard on January 3, 2018
LINK 2:What Is a Hepatobiliary (HIDA) Scan And How Is It Conducted?
https://www.medicalhealthtests.com/medical-tests/hepatobiliary-scan.html
Submitted on March 27, 2012
LINK 3: What Is a HIDA Scan with CCK?
https://www.wisegeek.com/what-is-a-hida-scan-with-cck.htm
by Mary McMahon (with figures, pix)
Last Modified Date: November 23, 2020
LINK 4: Radiology Questionnaire, 1 page
https://ereferrals.bcbsm.com/bcn/news-archive/
pdf/Questionnaire_MRI_NuclearHIDA.pdf
Blue Care Network of Michigan
February, 2012
Technetium-99M DISIDA (200 MBq) was injected.
2020-11-27--Calgary Foothills Medical Centre.
In general, the HIDA test has been replaced by high quality ultrasound of the liver and gallbladder.
However, in some situations it can be a valuable test to evaluate liver and gallbladder functional status.
A HIDA scan, also called cholescintigraphy or hepatobiliary scintigraphy,
is an imaging test used to view the liver, gallbladder, bile ducts, and small intestine.
The scan involves injecting a radioactive tracer into a person�s vein.
The tracer travels through the bloodstream into the body parts listed above.
A special camera takes pictures to track the tracer�s movement and transmit images onto a computer screen for observation and diagnosis.
To prepare for a HIDA scan, a person may need to fast for 4 to 12 hours before the scan.
After the scan .. A person should drink plenty of water to help speed up the radioactive tracer�s movement out of the body through urination and bowel movements.
A HIDA scan may be done to:
- measure the rate at which the gallbladder releases bile,
----- commonly referred to as gallbladder ejection fraction
- check the liver�s bile-excreting function
- follow the path of bile from the liver to the small intestine
- assess the outcome of a liver transplant
- find the cause of pain originating in the right side of the abdomen
- uncover the cause of jaundice or a yellowish hue to the skin
HIDA scans can help diagnose the following:
- biliary atresia, a rare congenital or inherited bile duct abnormality
- cholecystitis or inflammation of the gallbladder
- complications of operations, such as bile leaks or fistulas,
----- which are abnormal connections between two organs obstruction of the bile duct
During the procedure:
- The person will lie down on a table and be instructed to remain still throughout the scan.
- A specialist will insert an intravenous (IV) line into the person�s arm or hand and inject a radioactive tracer.
The person may experience a slightly cold sensation, which may feel like one is urinating, or feeling of pressure while this is happening.
- A technician will position a gamma camera above the person�s stomach to capture images.
- The tracer will move through the IV line into the bloodstream.
From there, it will travel to the liver. At this stage, bile-making cells in the liver absorb the tracer and carry it through the gallbladder, bile duct, and small intestine. This process may take approximately 60 to 90 minutes, although it can take up to 4 hours in some cases.
- A technician will control the camera, and a radiologist will view the images on a screen.
Results
HIDA scan results can be classed as:
-
Normal:
This means the tracer moved freely from the liver into the gallbladder and small intestine.
-
Slow movement:
If the tracer moved slowly through the body, this might suggest an obstruction or blockage in the gallbladder or bile duct, or it indicates below optimal liver function.
-
Not present:
If there is no sign of the radioactive tracer in the gallbladder, it can be a sign of acute inflammation of the gallbladder or acute cholecystitis.
-
Low gallbladder ejection fraction:
If a person takes CCK to empty the gallbladder, yet the amount of the radioactive tracer leaving the gallbladder is abnormally low, it can indicate chronic inflammation of the gallbladder or chronic cholecystitis.
-
Radioactive tracer detected in other parts of the body:
In cases where the tracer makes its way to other areas of the body, it suggests a leak in the biliary system.
How much does it cost?
HIDA scans vary in price. In some cases, insurance may cover the cost.
Healthcare Bluebook quotes USA $1,120 as the fair price for a HIDA scan.
Hepatobiliary scan or HIDA scan is conducted to examine the functioning of the liver.
It checks if bile is being made and excreted, if the bile ducts or drainage system are functioning appropriately, and if there is any malfunction in the gallbladder.
Typically, a hepatobiliary scan is coupled with an ultrasound of the gallbladder for a comprehensive evaluation.
HIDA scan is also referred to as a hepatobiliary iminodiacetic acid scan or an NM hepatobiliary scan.
This scan is an imaging process through which your doctor can track bile movements, its production and its flow into the small intestines from you liver. Basically, this scan generates pictures of your biliary tract, liver, gallbladder, and small intestine. It falls under the imaging study called nuclear medicine scans (NM scans). Nuclear medicine scans use a tracer, which are radioactive chemicals to highlight particular organs in the imaging scans.
The liver is one of the most complicated organs of the human body.
This organ is responsible for many different functions including some functions on which the life of the individual depends. No person can live without a liver that is partially functional. One of the many different functions of the liver is the production of bile. Bile is a fluid that is used to break down fatty foods in the digestive system. This fluid is produced in the liver and passed into the gall bladder where it is stored until the individual needs to digest food.
When digestion takes place, bile flows directly from the liver into the small intestine.
At the same time, bile from the gall bladder will also enter the area.
This increases the amount of bile available, thus ensuring that even large quantities of food get broken down effectively.
What Is a Hepatobiliary Scan?
The hepatobiliary scan is a scan used to determine the effectiveness of the liver�s functioning, particularly relating to its production and release of bile. A person may even have to go through a hepatobiliary scan with gallbladder ejection fraction in certain cases. The hepatobiliary scan is a nuclear medicine scan. This means that a radioactive tracer substance needs to be injected into the body. Tracer substances are used to mark out various organs and tissues in the body. This makes it possible for them to be seen clearly on any subsequent scan. The liver is used to filter out waste products from the blood. Thus, the tracer material will make the parts of the liver very clear in any scan.
The hepatobiliary scan is done in order to check if there is any obstruction in the bile ducts of the liver.
This scan is also done to check if there is any obstruction or inflammation of the gall bladder.
There may even be a situation where bile leaks into the intestines when it is not needed for digestion.
This sort of test will be able to determine if that is the case.
As the procedure begins, you would need to be in the supine position.
A radioactive chemical (tracer) will be injected through an IV line in a vein in your arm.
Cameras will be positioned over the table, above your gallbladder, to be precise, and images will be recorded for 60 to 90 minutes. The injected tracer will highlight areas of the gallbladder and make it visible to the NM camera.
The camera captures images every few minutes to track gallbladder enlargement.
This takes about an hour after which, CCK is injected to contract your bladder thereby highlighting gallbladder functioning for image capture.
INDEX
| {kind=link}
{kind=link}
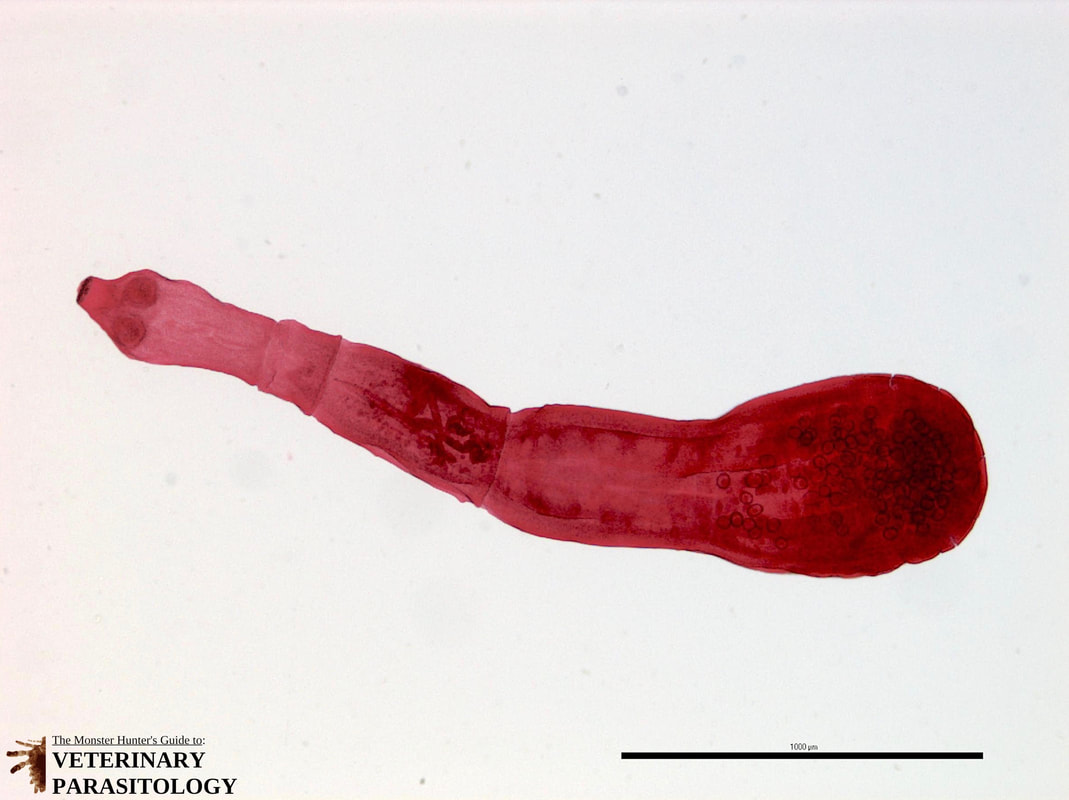{kind=link}
{kind=link}
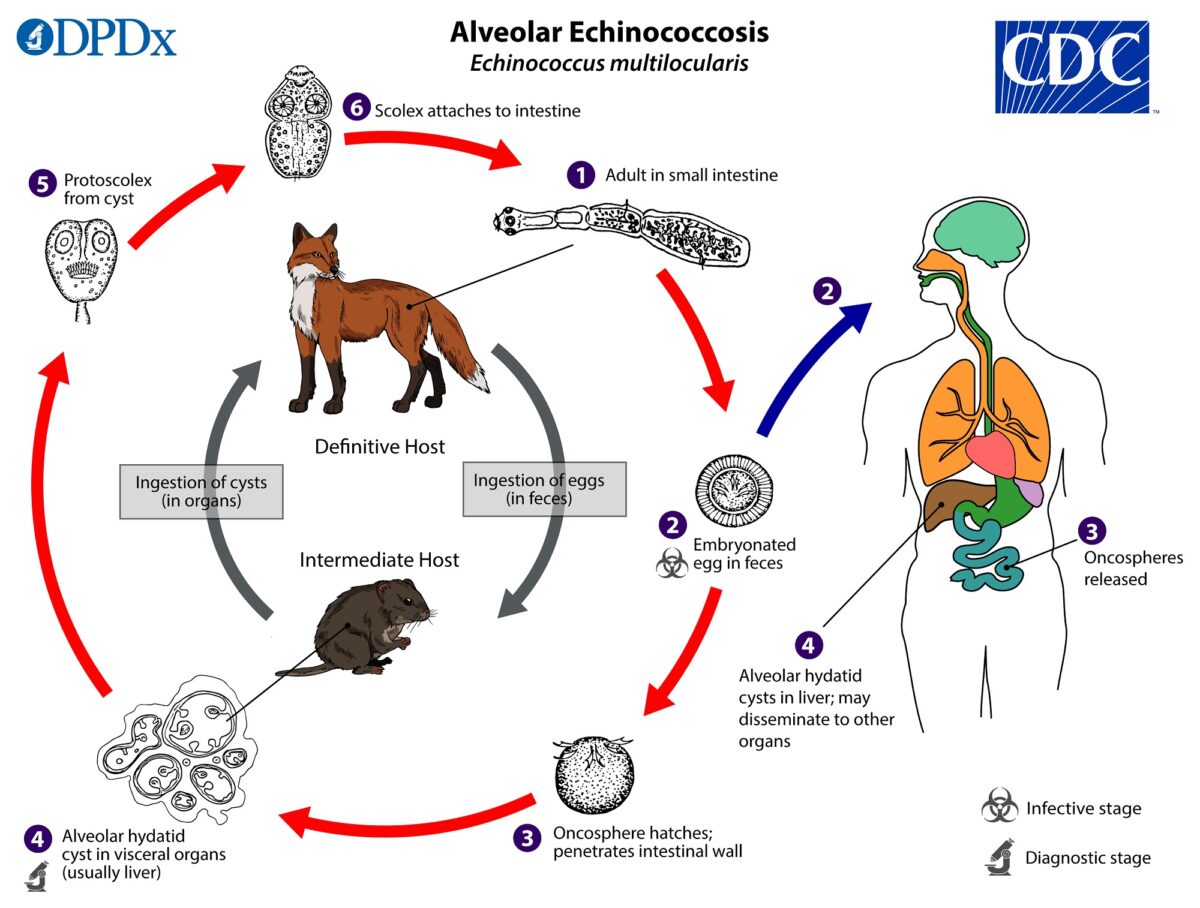{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}